
Today we’re back with another stop on our Fellows’ Case Files journey and making our way to the University of Rochester. Tune in to hear about this fascinating case and learn some key teaching points along the way.
Meet Our Guests
Dr. Shiv Patel completed his IM residency and a Chief year at the California Pacific Medical Center- Van Ness Campus and is currently a second-year PCCM fellow at the University of Rochester.
Dr. Mary Anne Morgan is an Associate Professor of Medicine and the Fellowship Program Director for the PCCM Fellowship at the University of Rochester. Her clinical interests range from the care of critically ill patients in the ICU to the diagnosis and management of rare lung disease in her role as Director of the University of Rochester LAM Clinic. She loves unwrapping clinical reasoning with trainees, exploring issues around communication and teamwork in the ICU, and is excited about curriculum revitalization in the growing URMC PCCM fellowship program.
Case Presentation
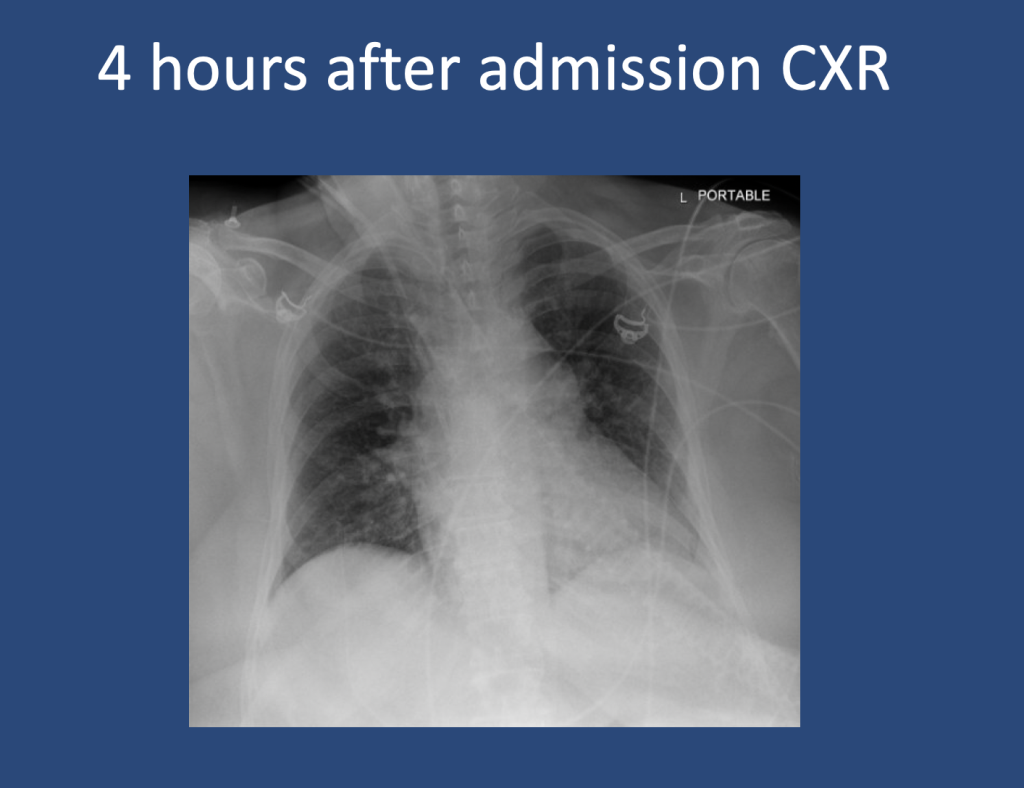
A 75 y.o. female with a history of Hypertension, Hyperlipidemia, and Type 2 Diabetes presented for evaluation of hypoglycemia and generalized fatigue. She had felt poorly for about a week with symptoms of back pain, generalized weakness, and dyspnea, all of which acutely worsened on the day of presentation.
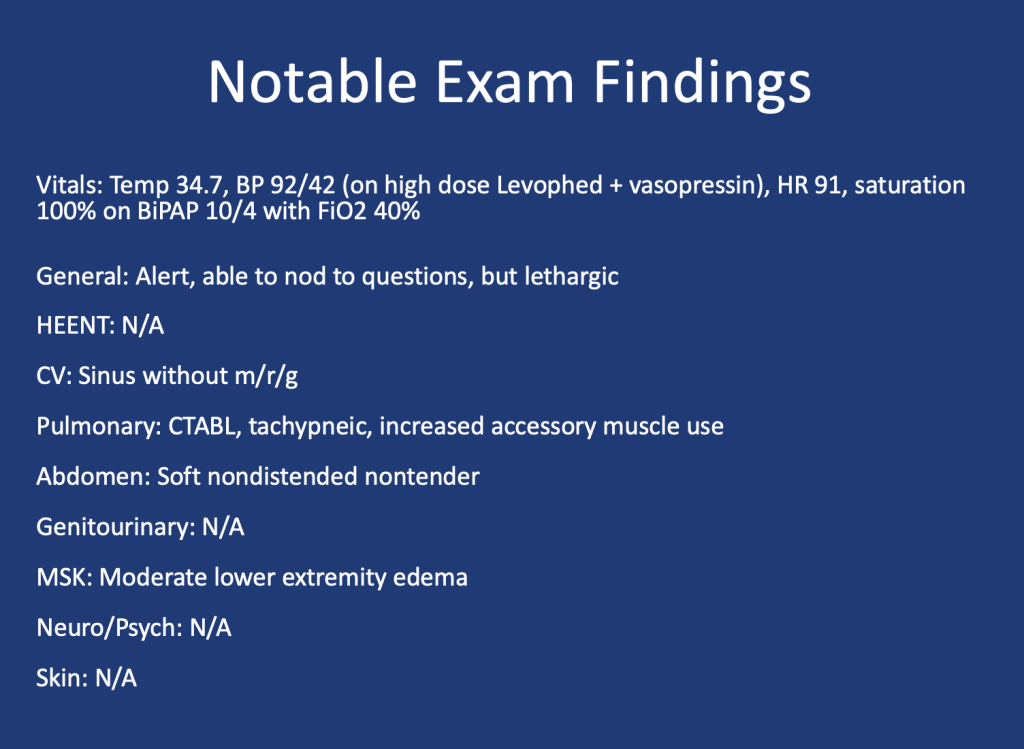
She was found to be hypoglycemic with a blood glucose level in the to 40’s. Initial vital signs included a heart rate of 56, blood pressure of 70/40, respiratory rate of 30, and temperature of 28.5 degrees Celsius.
Key Learning Points
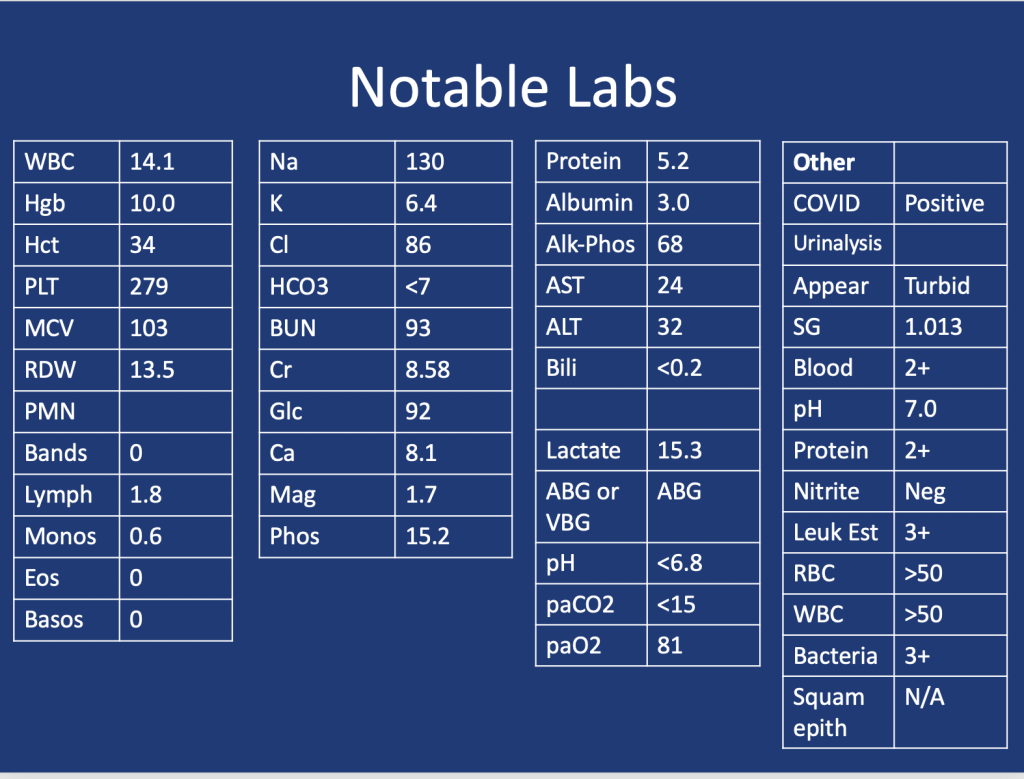
Lactic Acidosis: Type A, Type B and Type D
Type A: Typically secondary to conditions that impair oxygen delivery (respiratory failure, PE) to tissues or decrease tissue perfusion (severe anemia, shock). Patients typically present with hypotension, tachycardia, tachypnea, altered mental status, and signs of organ dysfunction.
Type B: Typically secondary to conditions that directly affect cellular metabolism or lactate clearance and characterized by the presence of hyperlactatemia without evidence of tissue hypoperfusion or hypoxia. Conditions associated include liver dysfunction (e.g., liver failure, cirrhosis), malignancies (especially hematological malignancies), medications/toxins (e.g., metformin, cyanide poisoning), inborn errors of metabolism, and mitochondrial disorders.
Type D: Less common presentation and can be seen in patients with short gut syndrome.
References
1.Blough B, Moreland A, Mora A Jr. Metformin-induced lactic acidosis with emphasis on the anion gap. Proc (Bayl Univ Med Cent). 2015 Jan;28(1):31-3. doi: 10.1080/08998280.2015.11929178. PMID: 25552792; PMCID: PMC4264704.
2.Callelo et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. DOI: 10.1097/CCM.0000000000001002
3.Friesecke, S., Abel, P., Roser, M. et al. Outcome of severe lactic acidosis associated with metformin accumulation. Crit Care 14, R226 (2010). https://doi.org/10.1186/cc9376
4.Madias NE. Lactic acidosis. Kidney Int. 1986 Mar;29(3):752-74. doi: 10.1038/ki.1986.62. PMID: 3702227.
5. Stiller RH, Luks AM, Çoruh B. All That Raises Lactate Is Not Sepsis. ATS Sch. 2023 Jun 12;4(3):385-386. doi: 10.34197/ats-scholar.2023-0032OT.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS | More