After a brief hiatus, we are excited to be back today with another Fellows’ Case Files! Today we’re virtually visiting the University of Kansas Medical Center (KUMC) to hear about a fascinating pulmonary presentation. There are some fantastic case images and key learning points. Take a listen and see if you can make the diagnosis along with us. As always, let us know your thoughts and definitely reach out if you have an interesting case you’d like to share.
Meet Our Guests
Dr. Vishwajit Hegde completed his internal medicine residency at University of Kansas Medical Center where he stayed for fellowship and is currently a second year Pulmonary and Critical Care medicine fellow.
Dr. Sahil Pandya is an Associate Professor of Medicine and Program Director of the PCCM Fellowship at KUMC.
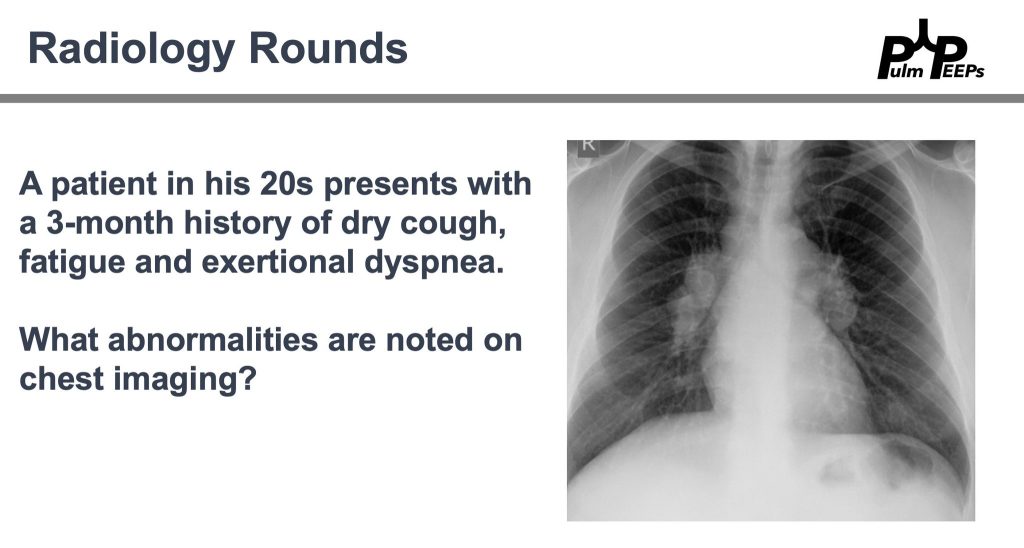
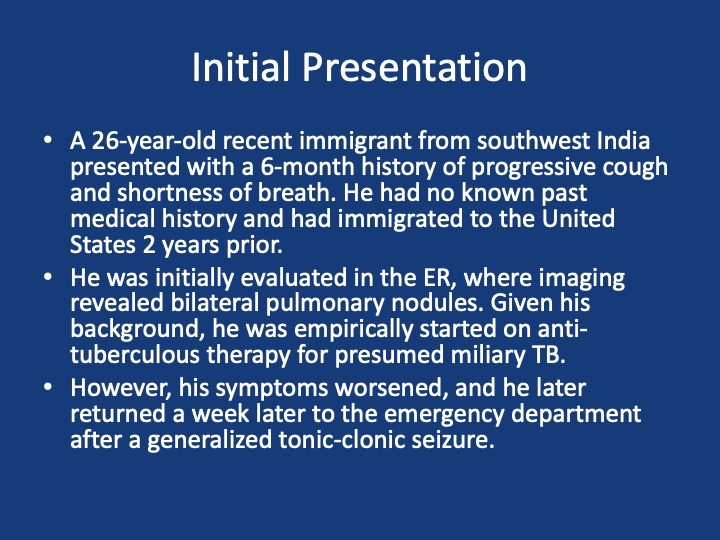
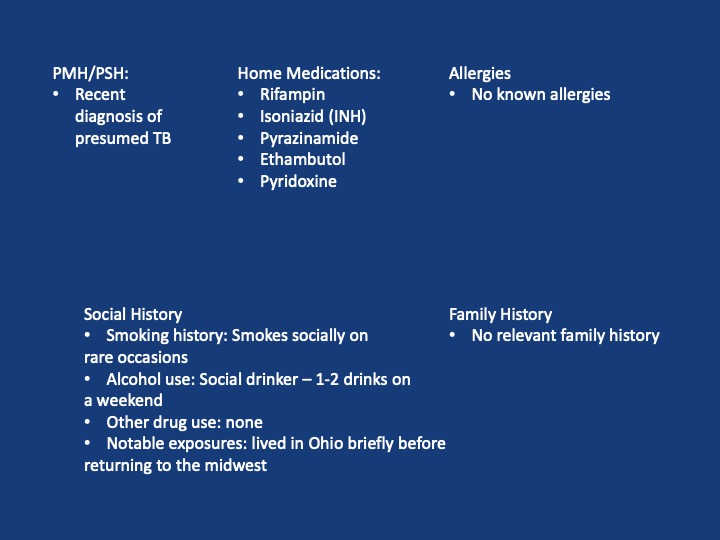
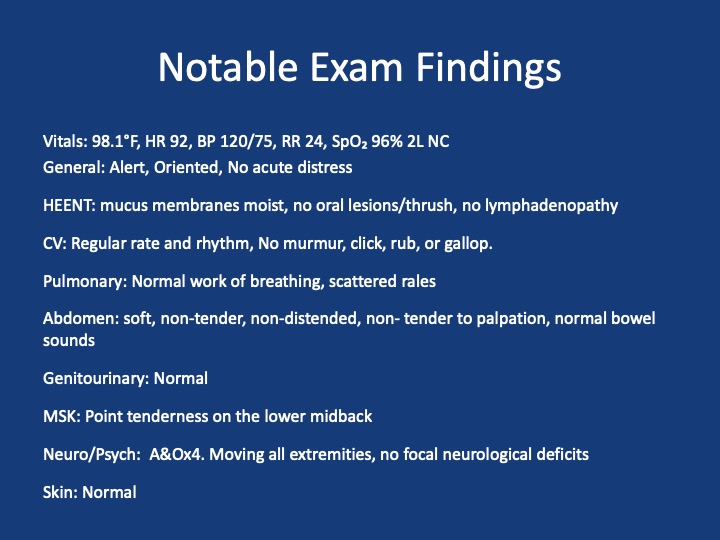
Case Presentation
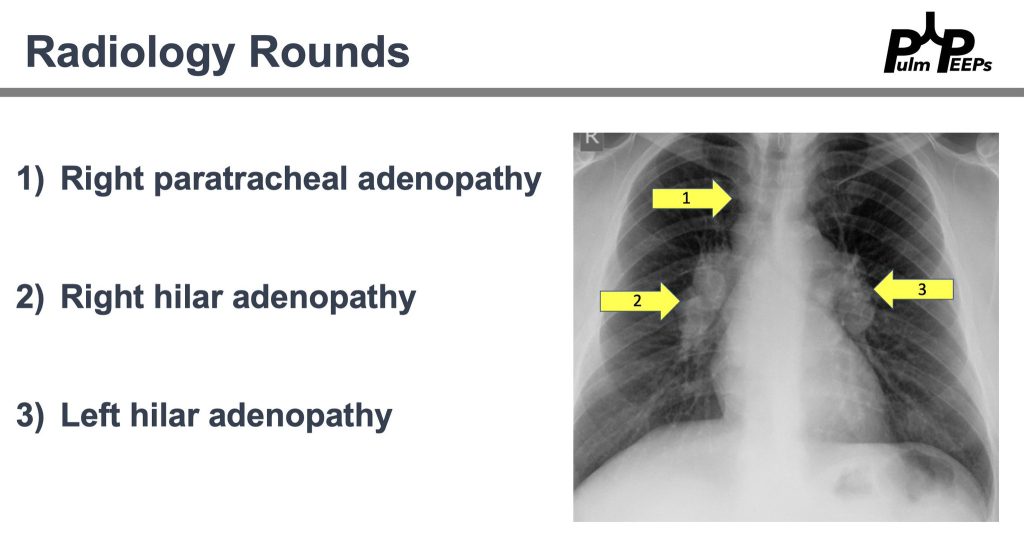
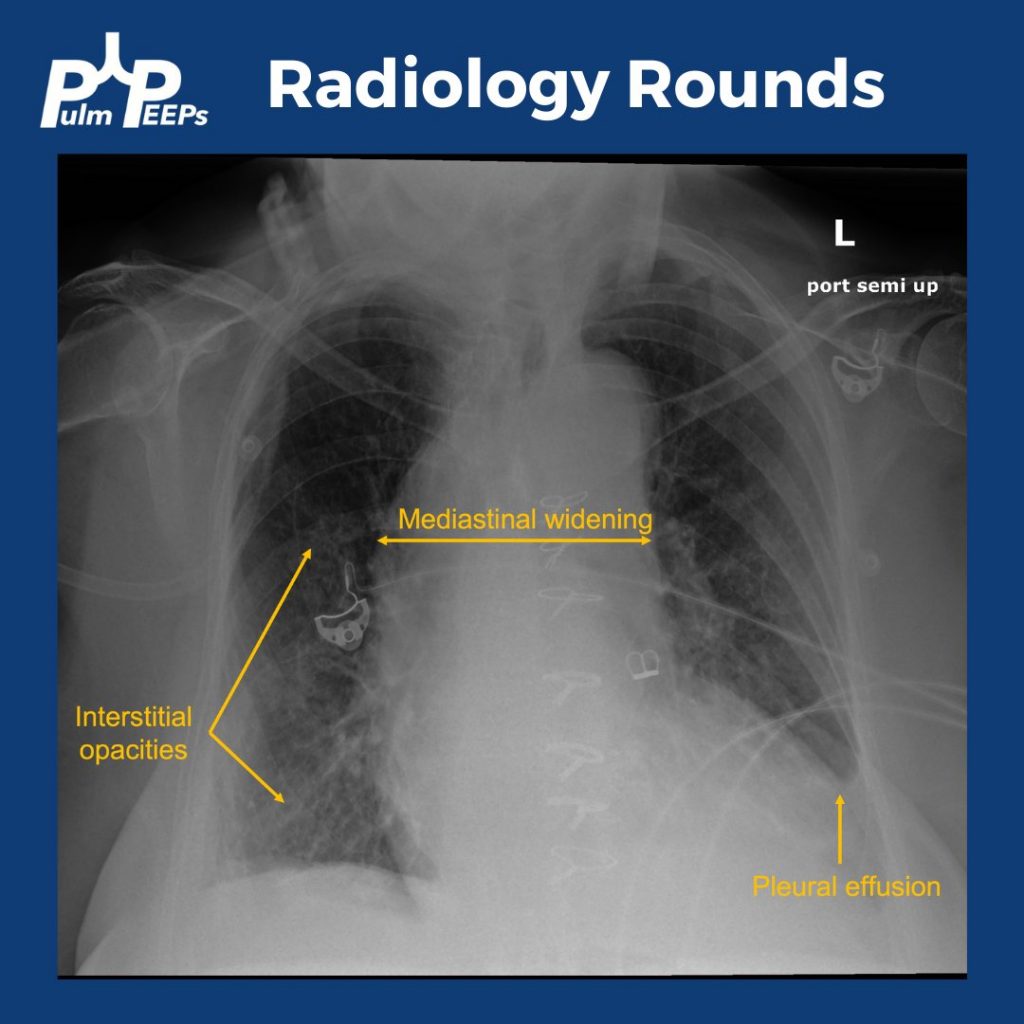
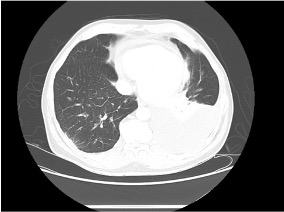
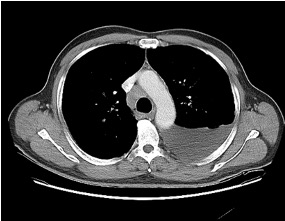
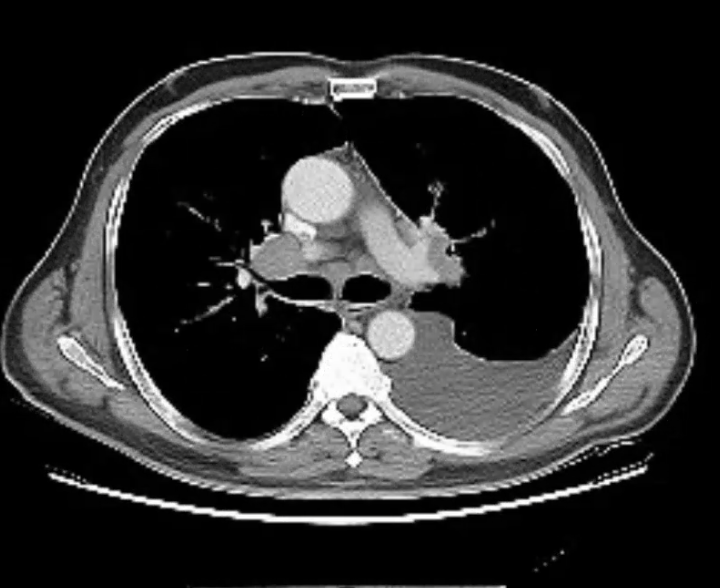
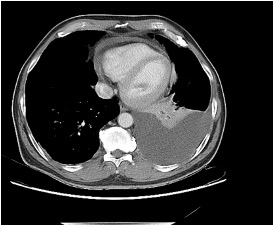
Imaging






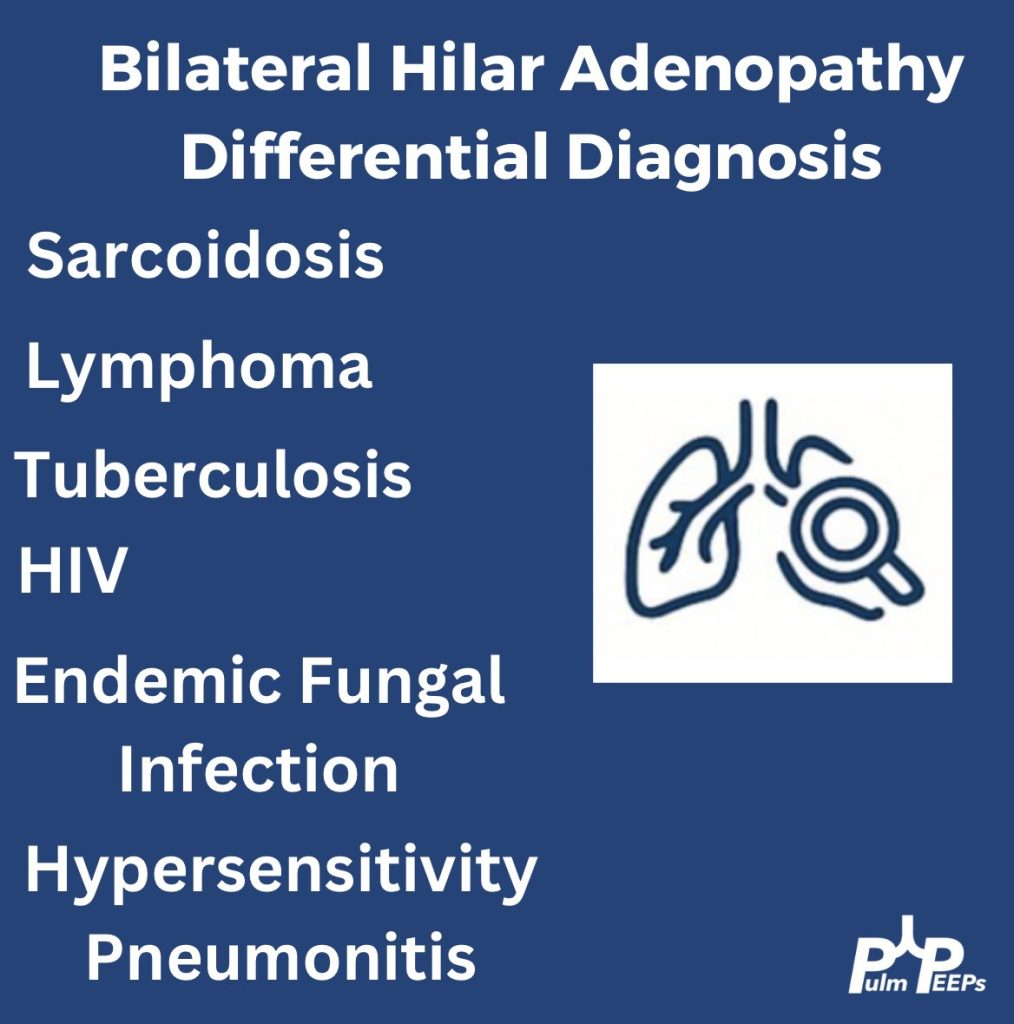
Infographic
Key Learning Points
1) Initial frame & diagnostic mindset
- Young (26), subacute → chronic dyspnea/cough with diffuse pulmonary nodules; avoid premature closure on TB.
- Use a Bayesian approach: combine pre-test probability (epidemiology, exposures, tempo) with targeted tests to decide next steps.
- Always confirm TB when possible (micro/path + resistance testing); empiric RIPE may be reasonable but shouldn’t replace tissue when stakes are high.
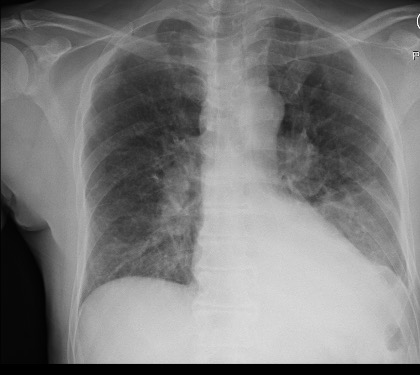
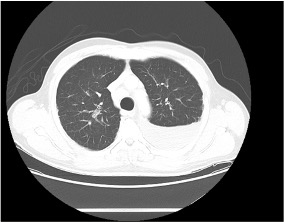
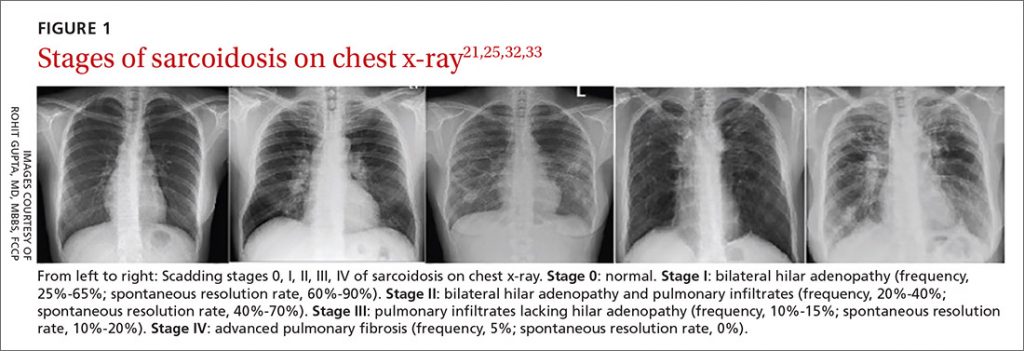
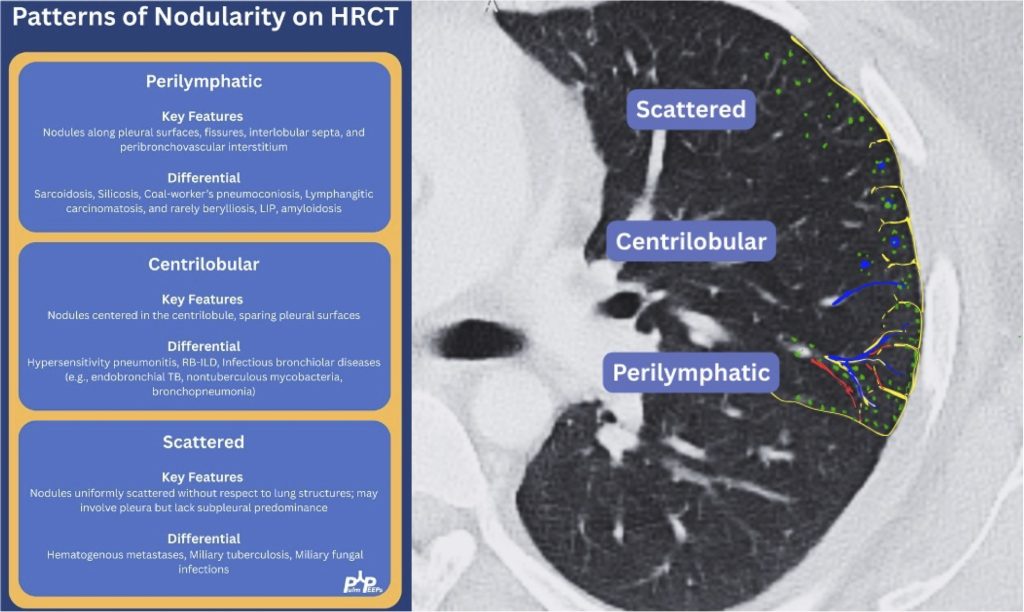
2) Imaging pearls—nodular pattern recognition
- Ask three things: craniocaudal distribution, symmetry, central vs peripheral.
- Centrilobular (spares pleura/fissures): airway-centered (e.g., NTM, bronchiolitis, tree-in-bud).
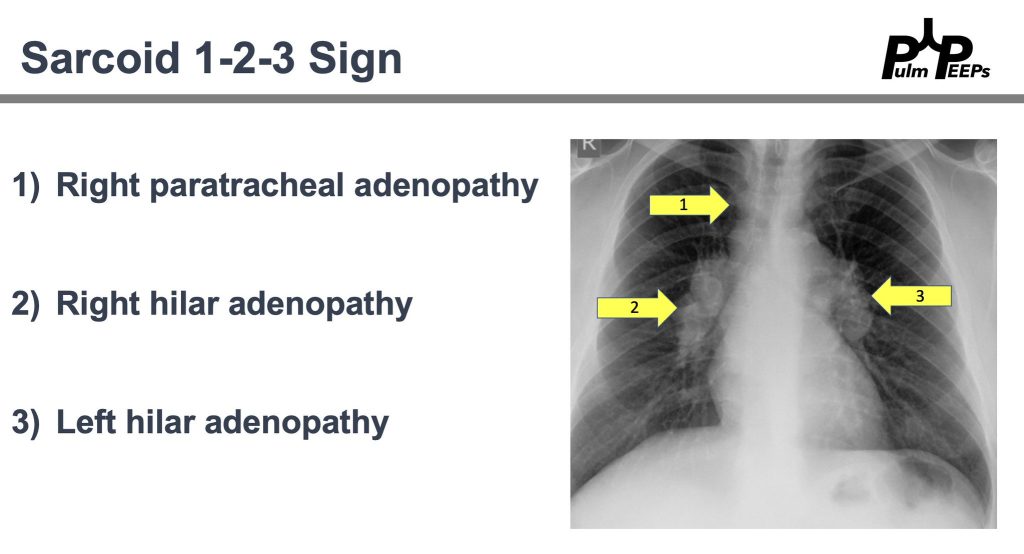
- Perilymphatic (tracks fissures/pleura & septa): sarcoid, lymphangitic spread.
- Random/diffuse (involves pleural surfaces): hematogenous spread → think miliary TB, disseminated fungal, septic emboli, metastatic disease.
- Interval change matters: new cavitation and confluence can upweight infection or aggressive malignancy.
3) Neuro findings—ring-enhancing lesions
- Differential: septic emboli/abscess, nocardia, fungal, TB, parasites, metastases, vasculitis, sarcoid.
- Partner with neuroradiology for pattern nuances; treat seizures but keep searching for the unifying diagnosis.
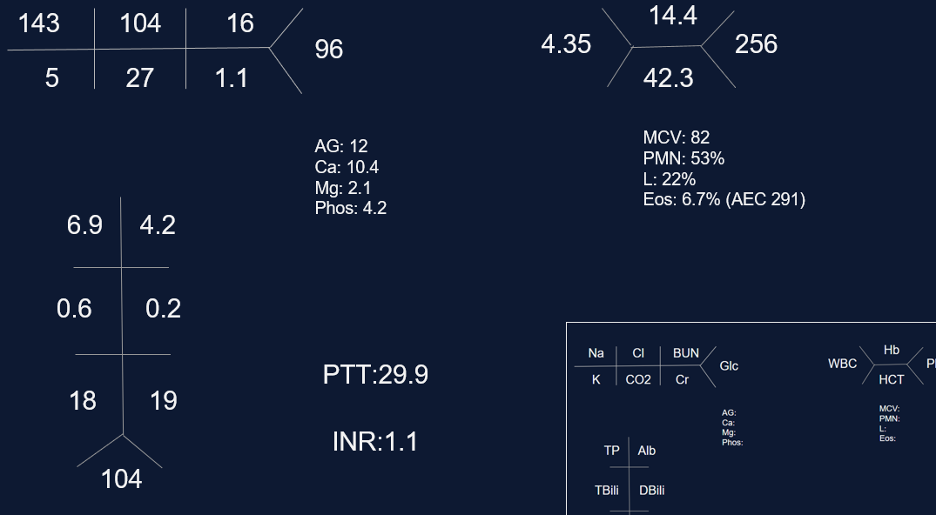
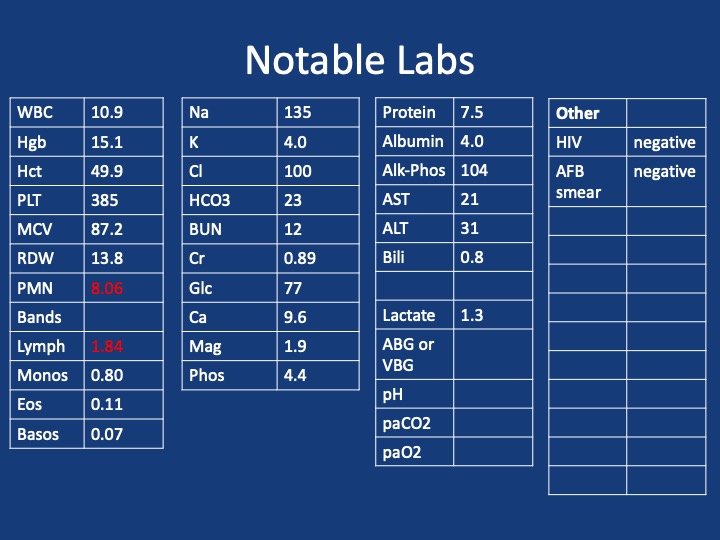
4) Lab/serology strategy
- Broad infectious workup (AFB × multiple, fungal serologies), HIV and basic immune screen.
- Negative/indeterminate tests don’t end the search—revisit history (e.g., Ohio travel → histo/blasto risk).
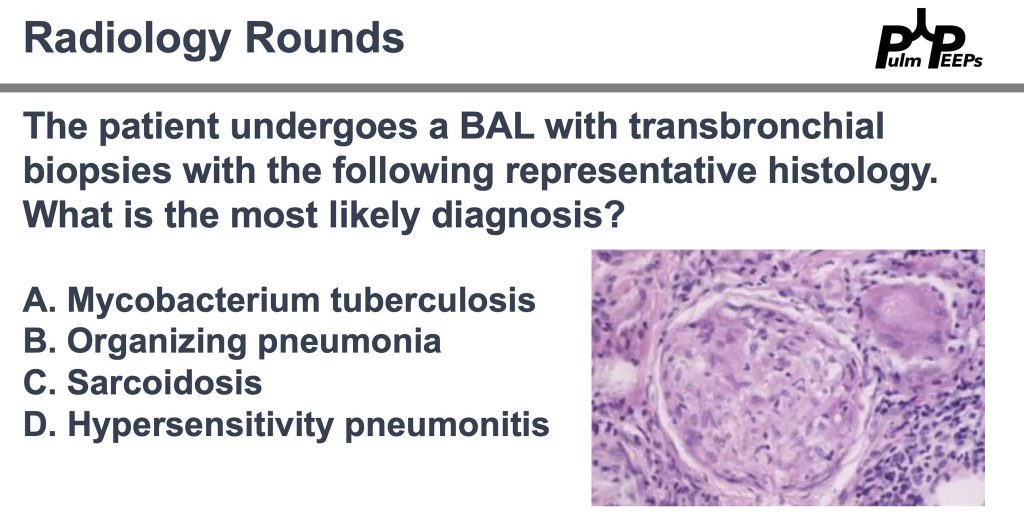
5) “Tissue is the issue”—choosing the procedure
- For diffuse nodules with mediastinal adenopathy and stable patient: EBUS-TBNA + BAL, consider transbronchial or cryobiopsy.
- Cryobiopsy pros: larger, less crush artifact, better for molecular testing; cons: ↑ bleeding/pneumothorax vs forceps.
- VATS still best for certain ILD questions or if less invasive routes are non-diagnostic—but weigh patient preference and stage/likelihood of yield.
6) ROSE (rapid on-site evaluation) in bronchoscopy
- Confirms adequacy in real time, steers you away from necrotic zones, helps decide when you’ve got enough for molecular studies, and when to pivot sites—reduces anesthesia time and repeat procedures.
7) Final diagnosis & management
- Path: TTF-1+, CK7+, napsin A → pulmonary adenocarcinoma with a fusion driver.
- Therapy: Targeted TKI (crizotinib) → dramatic radiographic response of miliary lung disease and CNS lesions.
- Teaching point: even “miliary TB-like” lungs + CNS lesions in a 20-something can be driver-positive lung cancer—don’t let age or pattern blind you.
References and Further Reading
- Desai, S., Devaraj, A., Lynch, D., & Sverzellati, N. (2020). Webb, Müller and Naidich’s high-resolution CT of the lung (6th ed.). Lippincott Williams & Wilkins.
- Rajeswaran, G., Becker, J. L., Michailidis, C., Pozniak, A. L., & Padley, S. P. G. (2006). The radiology of IRIS (immune reconstitution inflammatory syndrome) in patients with mycobacterial tuberculosis and HIV co-infection: appearances in 11 patients. Clinical radiology, 61(10), 833-843
- Poletti, V., Ravaglia, C., & Tomassetti, S. (2016). Transbronchial cryobiopsy in diffuse parenchymal lung diseases. Current opinion in pulmonary medicine, 22(3), 289-296.
- Norman, G. R., Monteiro, S. D., Sherbino, J., Ilgen, J. S., Schmidt, H. G., & Mamede, S. (2017). The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 92(1), 23-30.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS