Sidra Bonner is a general surgery resident at Michigan Medicine. She completed her undergraduate education at Cornell University and medical education at the University of California-San Francisco. Sidra also has a Master’s in Public Health focused in Health Policy from Harvard and a Master’s in Science Health and Healthcare Research from the University of Michigan. She is interested in pursuing a career in general thoracic surgery with a research focus aimed at addressing the multi-level contributors to racial and ethnic inequities in access, quality, and outcomes of surgical care for patients with lung and esophageal cancer.
Tom Valley is an Associate Professor in the Division of Pulmonary and Critical Care Medicine at the University of Michigan. He completed his IM residency and chief residency at the University of Texas-Southwestern/Parkland Memorial Hospital and then joined the University of Michigan as a pulmonary and critical care fellow in 2013 and stayed on for faculty and is the physician-lead for the University of Michigan Schwartz Rounds for Compassionate Care. Tom’s research aims to understand and improve medical decision making in the intensive care unit.
We are thrilled to be back with another episode in our Top Consults series. We are talking about Solitary Pulmonary Nodules, which is something every pulmonologist will encounter in the clinic and on in-patient consults. We go through a number of cases and provide a framework for approaching these cases.
Meet our guests
Dr. Jessica Wang Memoli is board certified in pulmonary disease, critical care medicine and internal medicine. She is the Director of Bronchoscopy and Interventional Pulmonary, as well as the Associate Fellowship Program Director for Pulmonary Critical Care Medicine at the MedStar Washington Hospital Center. Dr. Wang Memoli received her medical degree from the University of Miami Miller School of Medicine. She completed her residency at MedStar Washington Hospital Center and her fellowship training at the Medical University of South Carolina in Charleston.
Dr. Nick Ghionni works at Union Memorial, Good Samaritan, and Franklin Square as an Intensivist and Pulmonologist. He completed his Internal Medicine residency at Mercy Catholic Medical Center in PA serving as Chief Internal Medicine resident. He was a fellow at MedStar Washington Hospital Center where he was the Chief Pulmonary Critical Care Fellow. His specific interests include mechanical ventilation, POCUS, and medical education.
Case Presentations
Case 1:
33 year old woman who came to the emergency department with acute onset of shortness of breath. She states that she had been in her normal state of health until this morning when she developed shortness of breath at rest, and chest pain. She does report a non-productive cough over the last few weeks which she feels may be contributing to her chest pain. She does report a history of asthma during childhood but without any exacerbations or maintenance therapies needed during her adulthood. She does report wheezing when she is sick with a cold but this is infrequent. The ED team sent off an initial work-up including a D-Dimer which was elevated, and she underwent a CTA of the chest for concern for possible PE. On the CT scan, there was no PE but the radiologist did call a “2 mm indeterminate right upper lobe pulmonary nodule.”
Case 2:
We have a 67-year-old male with a past medical history of ischemic cardiomyopathy, chronic systolic heart failure (LVEF 10-15%), s/p AICD, diabetes mellitus type 2, hyperlipidemia, hypertension, chronic kidney disease stage III, prostate cancer s/p seed implantation that was over 15 years ago who presented with acute decompensation of his heart failure and cardiogenic shock. He was successfully managed for that and is now being worked up by advanced HF and as a part of that workup got a chest CT, which found a RUL 6 mm nodule.
Case 3:
We have a 66-year-old male with a past medical history of HTN and drug abuse who presented to the ED with acute SOB, likely a COPD exacerbation. He was given bronchodilator and steroids as well as being started on Bipap. He eventually was able to be weaned off Bipap and was able to tolerate nasal cannula. As a part of his initial work up, the patient underwent CT scan for possible PE which demonstrated a new LUL spiculated nodule that is 1.3cm that is new since 2019.
Key Learning Points
Approaching Pulmonary Nodules:
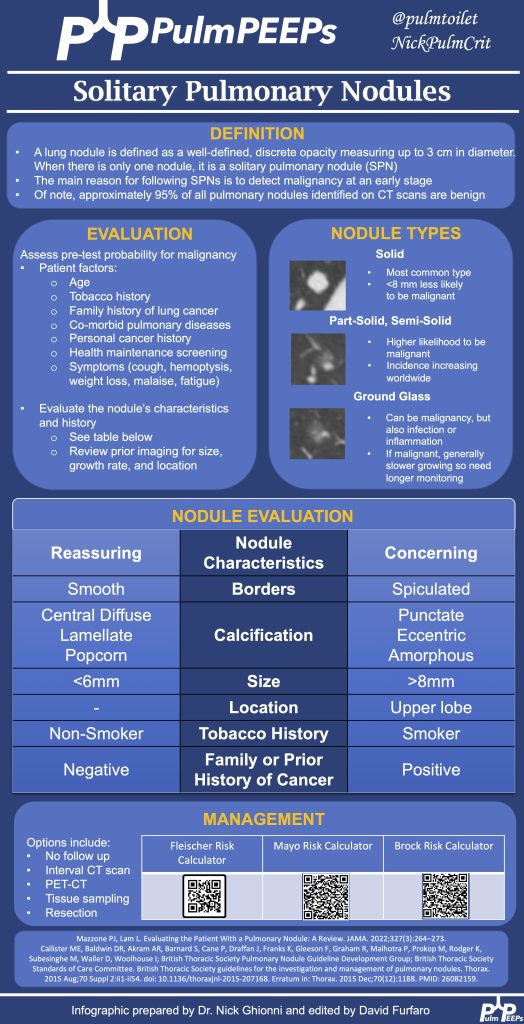
A structured approach is essential due to the complexities of diagnosing pulmonary nodules.
Patient history, including risk factors, past interventions, and imaging, plays a vital role.
Nodules’ appearance, such as location, shape, or characteristics like calcification or spiculation, can provide diagnostic clues.
The nodules history on serial imaging is a key predictive risk factor for determining the likelihood that the nodule represents cancer
Tools like the Mayo Risk Calculator and Fleishner Society guidelines assist in risk assessment and guidance.
It’s essential to assess patient risk, and nodule risk, and prioritize patient concerns and education. Periodic monitoring or follow-up might be necessary based on the nodule’s risk and size.
A multidisciplinary approach involving various specialists ensures comprehensive care.
Key Discussion Points:
PET Scans:
Useful in gauging a nodule or tumor’s metabolic activity.
Large, hypermetabolic nodules are suspicious.
Not every positive PET result means malignancy; other causes like inflammation or scars can produce positive results.
Evaluating Nodules:
Consideration of nodule size, characteristics, patient history, and risk calculators is crucial.
Tumor boards provide a collaborative expertise approach.
Tissue Sampling & Testing:
The method of tissue sampling depends on resources and expertise.
CT-guided biopsy offers a high diagnostic yield but with a risk of pneumothorax.
Bronchoscopic biopsy provides a lower diagnostic yield than CT-guided biopsy but has a significantly reduced risk of complications.
Advanced diseases now often require molecular testing on tissue samples.
Ground Glass Nodules:
Different from solid nodules due to their slow growth rate.
Monitoring is crucial due to the potential for transformations raising cancer suspicions.
The approach for ground glass nodules typically involves more extended monitoring intervals than for solid nodules.
Holistic Evaluation:
Consider the nodule’s characteristics, the patient’s history, and clinical intuition.
Individualized patient assessment is as vital as evidence-based guidelines and clinical expertise.
See the infographic for a summary of key learning points:
References and further reading
Loverdos K, Fotiadis A, Kontogianni C, Iliopoulou M, Gaga M. Lung nodules: A comprehensive review on current approach and management. Ann Thorac Med. 2019 Oct-Dec;14(4):226-238. doi: 10.4103/atm.ATM_110_19. PMID: 31620206; PMCID: PMC6784443.
Mazzone PJ, Lam L. Evaluating the Patient With a Pulmonary Nodule: A Review. JAMA. 2022 Jan 18;327(3):264-273. doi: 10.1001/jama.2021.24287. PMID: 35040882.
MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, Mayo JR, Mehta AC, Ohno Y, Powell CA, Prokop M, Rubin GD, Schaefer-Prokop CM, Travis WD, Van Schil PE, Bankier AA. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017 Jul;284(1):228-243. doi: 10.1148/radiol.2017161659. Epub 2017 Feb 23. PMID: 28240562.
Wahidi MM, Govert JA, Goudar RK, Gould MK, McCrory DC; American College of Chest Physicians. Evidence for the treatment of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 Sep;132(3 Suppl):94S-107S. doi: 10.1378/chest.07-1352. PMID: 17873163.
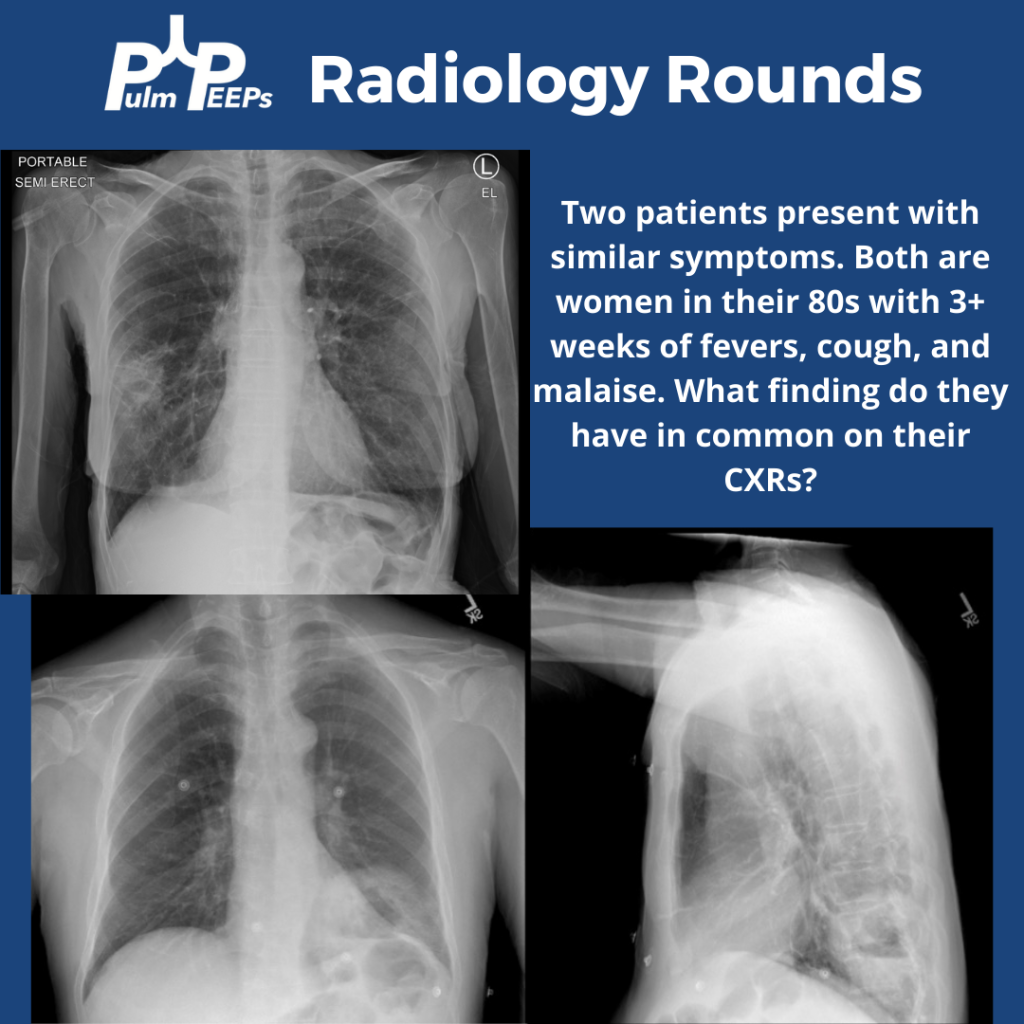
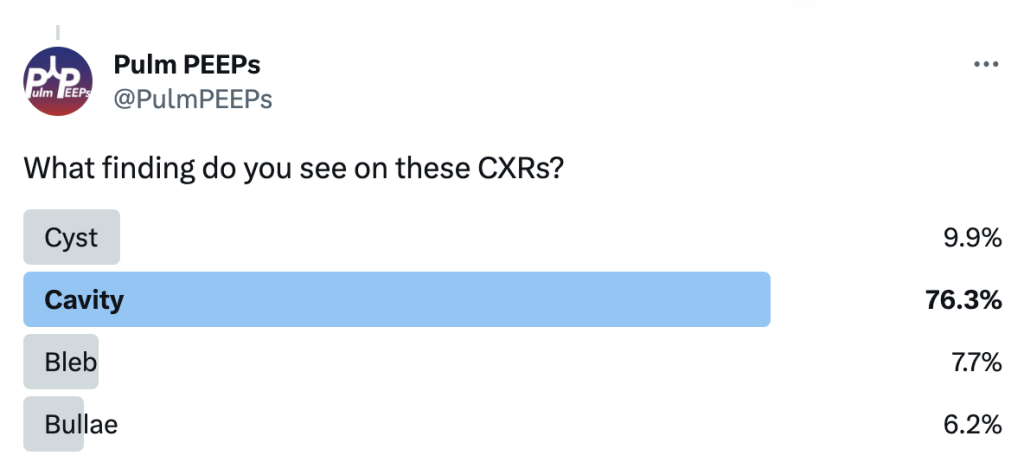
Tuesday is time for another #RadiologyRounds! Time for some CXR reading and a differential diagnosis mnemonic Two women presented to the hospital with similar presentations. They are both in their 80s with multiple weeks of cough, fever, and fatigue. Here are the CXRs
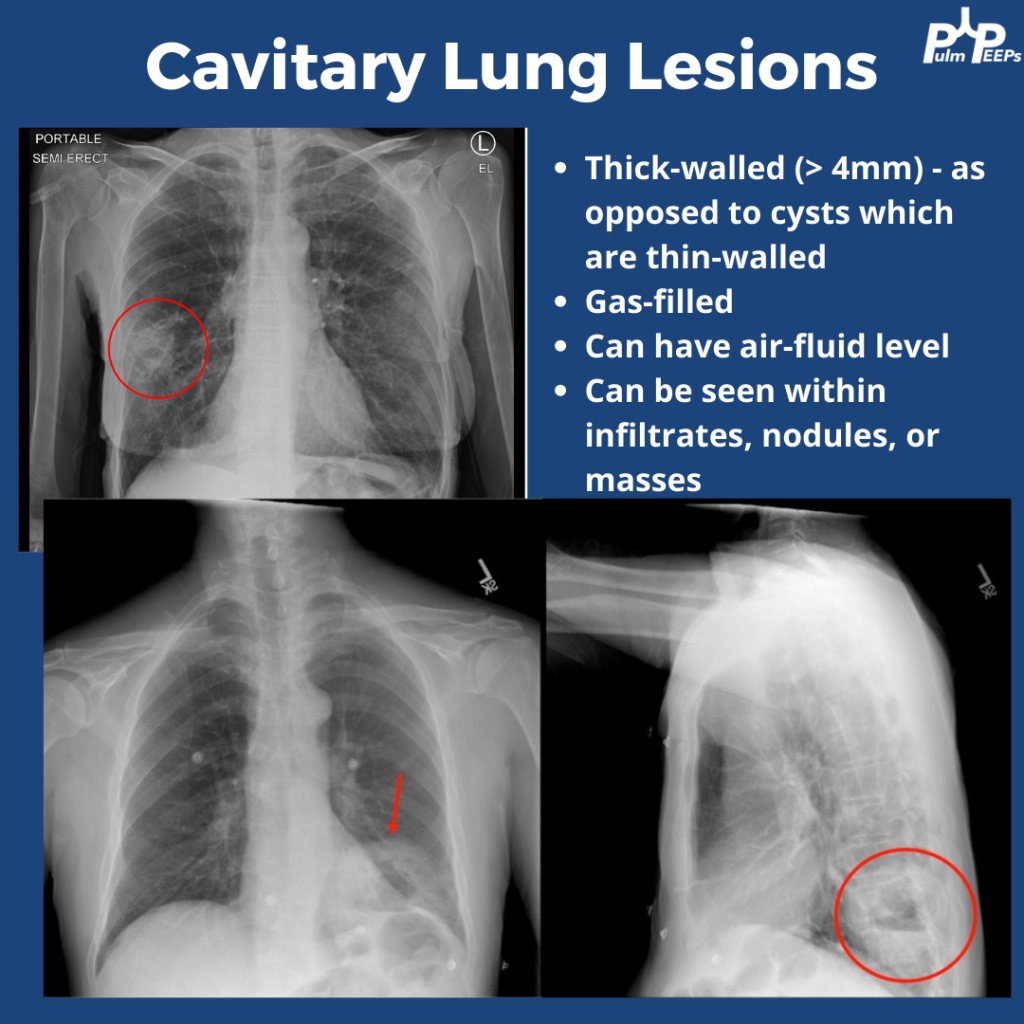
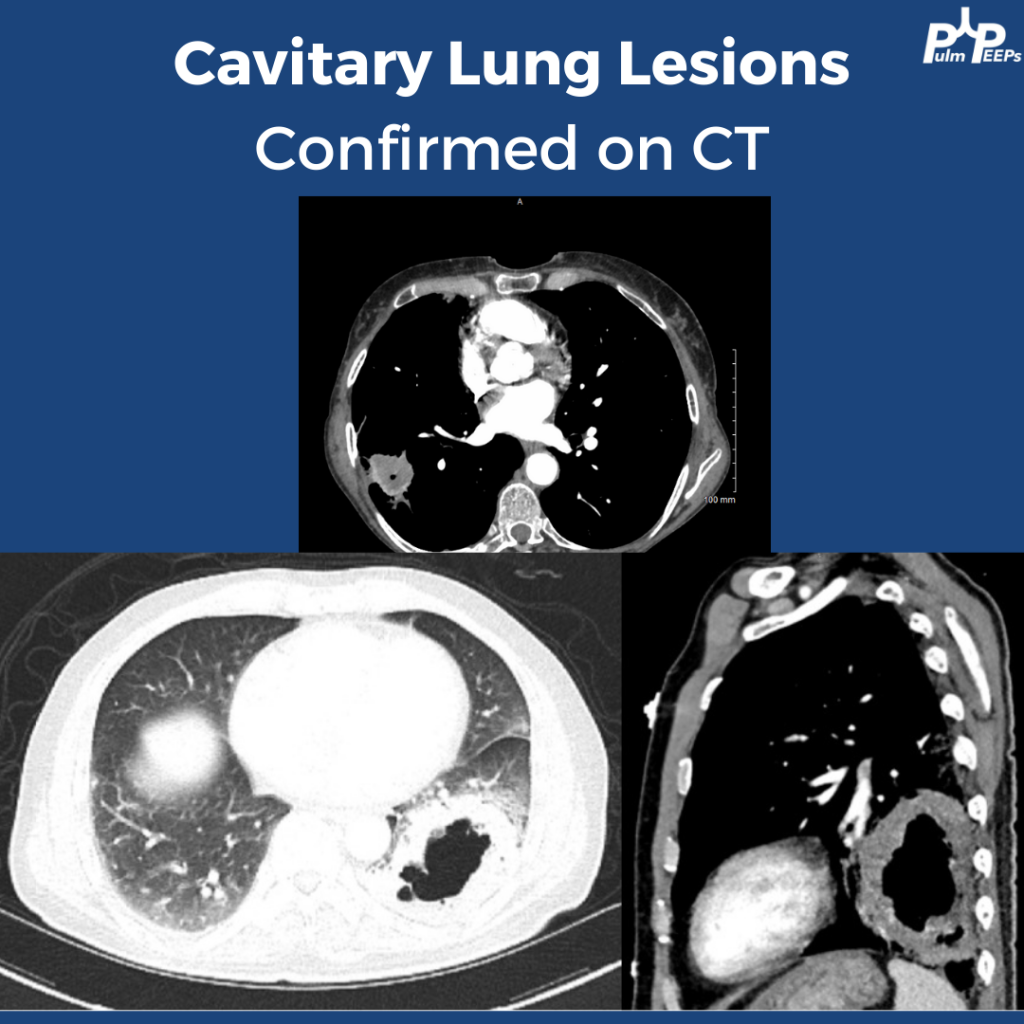
The CXRs both showed cavities. They are thick-walled (>4mm) and gas-filled. Cavitary lung lesions are seen within infiltrates, nodules, or masses. There can be an air-fluid level within the cavity. Cysts have thinner walls. The findings were confirmed on CT scan
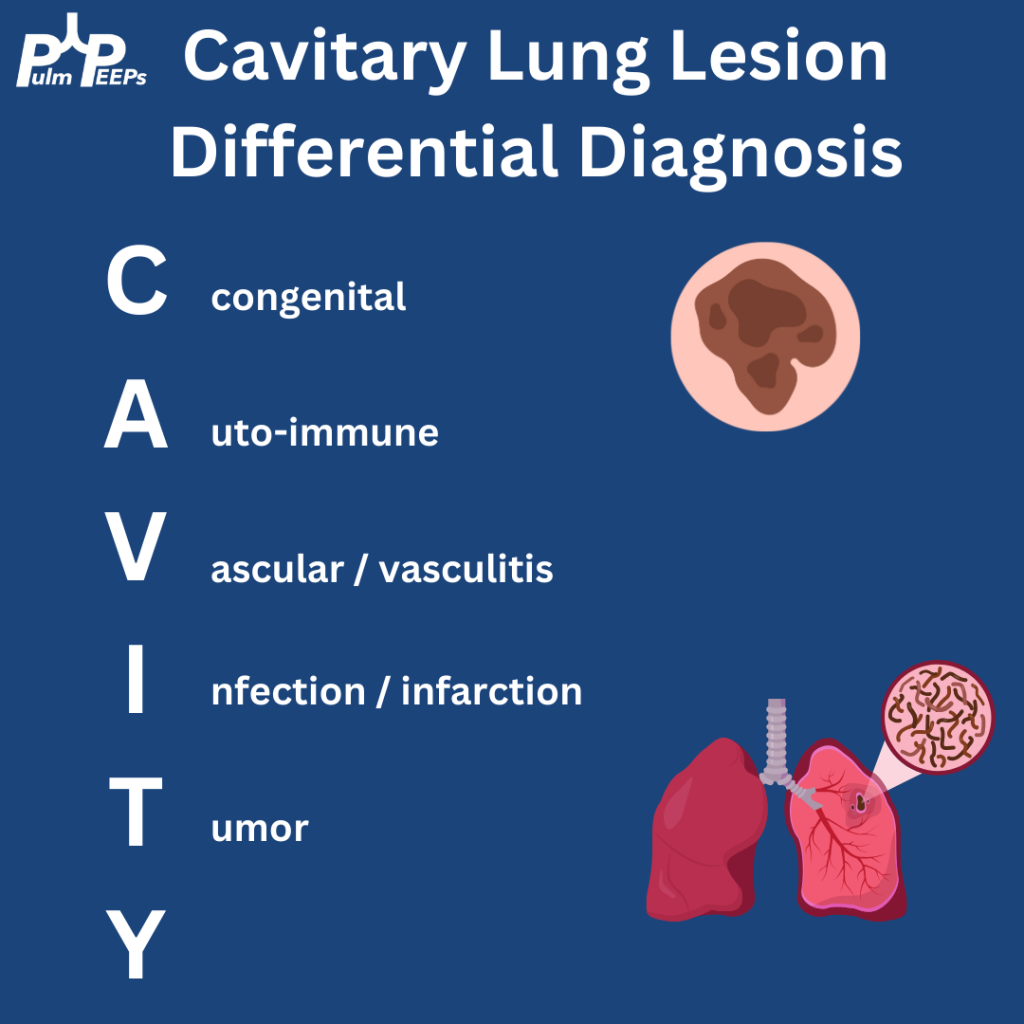
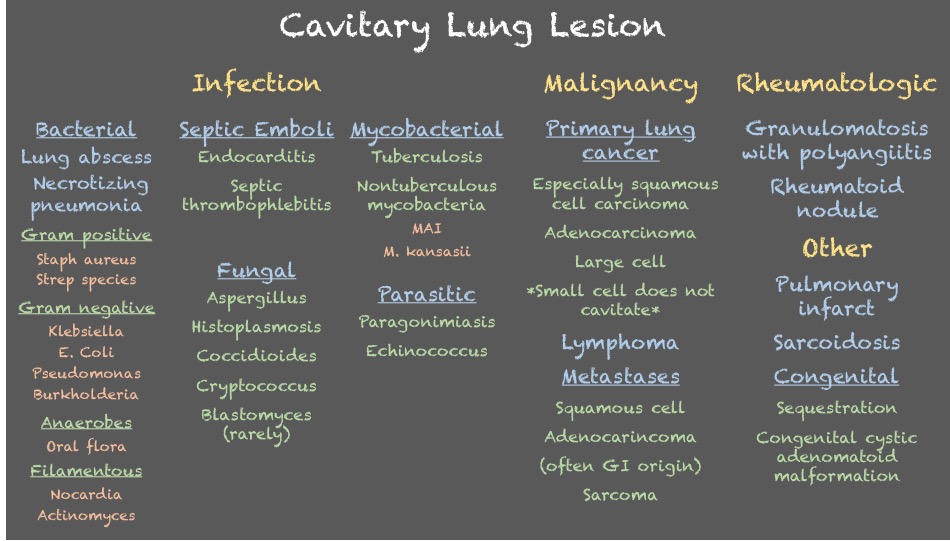
Cavitary lung lesions can have a broad differential so it is helpful to have a systematic approach. To make it easy, when you see this just remember: CAVITY
Bonus points to anyone who can fill in the Y
Both patients were ultimately diagnosed with pulmonary abscesses which improved with prolonged courses of antibiotics with anaerobic and gram-negative coverage.
We’re diving back into some pleural fluid today (okay that is kind of gross to think about and we apologize). If you haven’t listened to our prior pleural effusion episodes and want to start from the top, then check out Episode 36 for a general approach to pleural effusions, and Episode 37 to hear about parapneumonic effusions. Malignant effusions are another common consult question and we’ll talk about everything from detection to monitoring, to definitive management.
Meet Our Guests
Dr. David DiBardino is an Assistant Professor of Medicine at the University of Pennsylvania Medicine and is the Associate Director for Clinical Research within the Section of Interventional Pulmonology. He is also the Program Director for the Interventional Pulmonary Fellowship there.
Dr. Jamie Bessich is an Assistant Professor of Medicine and Cardiothoracic Surgery at NYU Grossman School of Medicine. She is the Section Chief of Interventional Pulmonology and is the Director of Bronchoscopy at Tisch Hospital.
Dr. Van Holden is an Associate Professor of Medicine at the University of Maryland School of Medicine and is the Pulmonary and Critical Care Fellowship Program Director there. She was last on the show for our very first Fellows’ Case Files when we discussed a fascinating case of pulmonary alveolar proteinosis.
Case Presentation
The page: 72M smoker, new effusion, concern for malignancy, tap?
Further history: 72 year old man with PMH of GOLD B COPD, tobacco use (55 pack years), HTN, HLD, and diabetes. He presented to the ED with progressive dyspnea and fatigue. He is on LAMA/LABA for his COPD, and he does not frequently have exacerbations. He has no increased sputum production or wheezing, but he has been feeling progressively fatigued and lethargic. H Over the past few weeks he has had more dyspnea on exertion, and now has it at rest too. It is a bit worse when he lies flat. He has had no weight gain or edema in his legs and has actually lost 10-15 pounds in the last 3 months. In the ED, he is newly requiring 3-4L NC, has decreased breath sounds on the right, and a CXR shows a large right-sided pleural effusion, as well as a large apical nodule with some spiculation, both of which are new from prior.
Key Learning Points
Causes of malignant pleural effusion
–Lung cancer is the most common in men
–Breast cancer is the most common cause in women
–Lung and breast cancer account for > 50% of all malignant pleural effusions
–Other less common causes are lymphoma, GU or GI tract cancer
–Remember to consider mesothelioma
Prognosis of MPE
–Malignant pleural effusion means the cancer is advanced and stage 4 by definition
–The average life expectancy after a diagnosis of MPE is 3-12 months, depending on the patient and the malignancy
Imaging and MPE
–Make sure to get a CT scan after drainage so no lesions are missed
–Ultrasound can be helpful to look for disruptions of the pleural line, loculated fluid, or pleural nodules
Pleural fluid analysis
–Make sure to send common labs (gram stain, culture, pH)
–Cell count is very important as most MPE are lymphocyte-predominant
–Triglycerides can be helpful as well (more on chylothorax in future episodes)
–Cytology is essential and makes the diagnosis. The sensitivity is 65 – 75 percent so repeat taps may be needed and you need to send at least 60 cc of fluid (often more)
–If you have high suspicion and no diagnosis after two taps, pleuroscopy and pleural biopsy is warranted
Management of MPE
–First you need to determine if the MPE is recurrent. This requires drainage and then monitoring
— The main options are repeat thoracenteses, pleurodesis, or indwelling pleural catheter. A combination can often be used, and shared decision making is essential to the determining the best option
–The three things to consider with recurrent malignant pleural effusion are:
Did the patient feel better after drainage?
Did the lung fully re-expand?
What is the best option for this specific patient to optimize quality of life and time outside of the hospital?
–In AMPLE, pleural cetehters and talc pleurodesis were compared, and both are reasonable options with equivalent outcomes on quality of life; although pleural catehters had fewer hospital days overall.
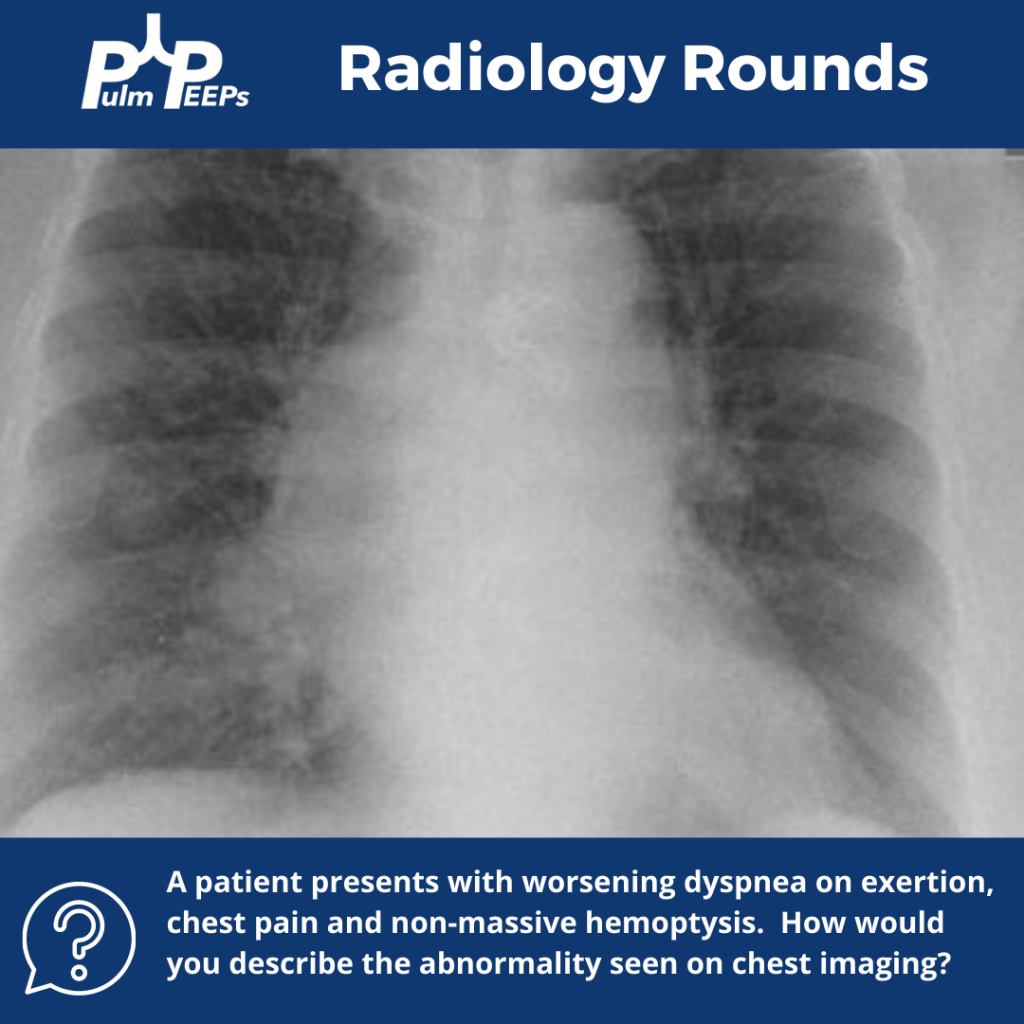
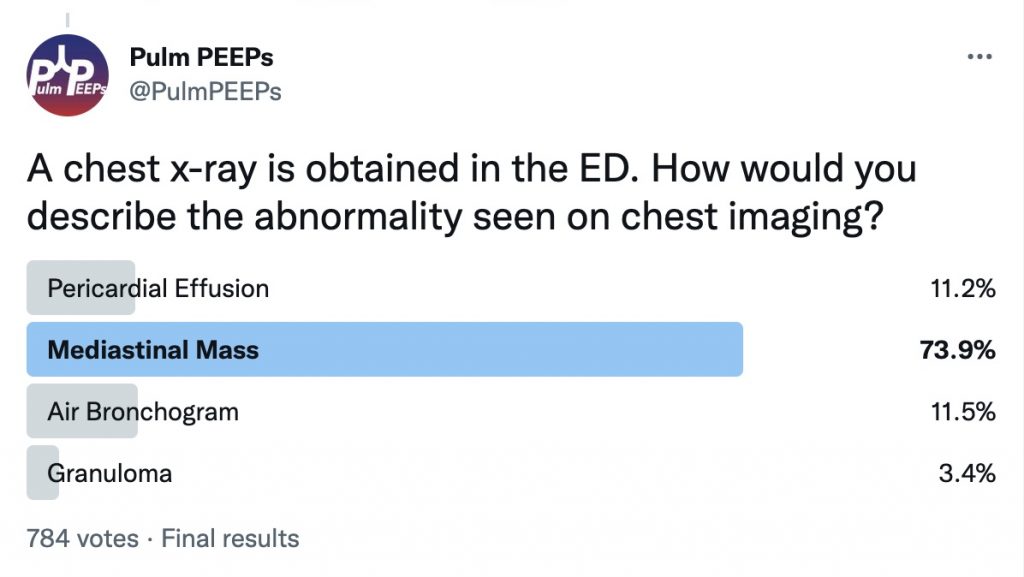
We’re excited to bring you another Radiology Rounds today that combines pulmonary and critical care.
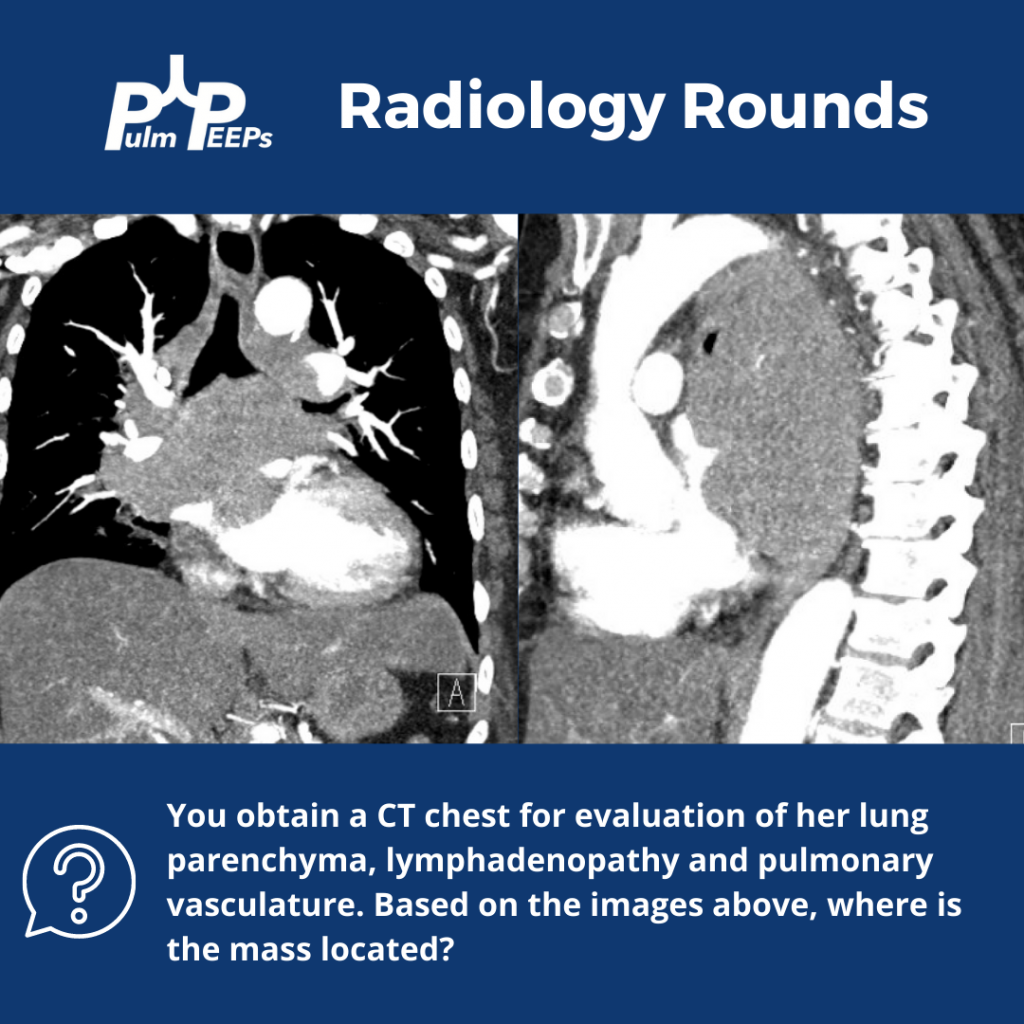
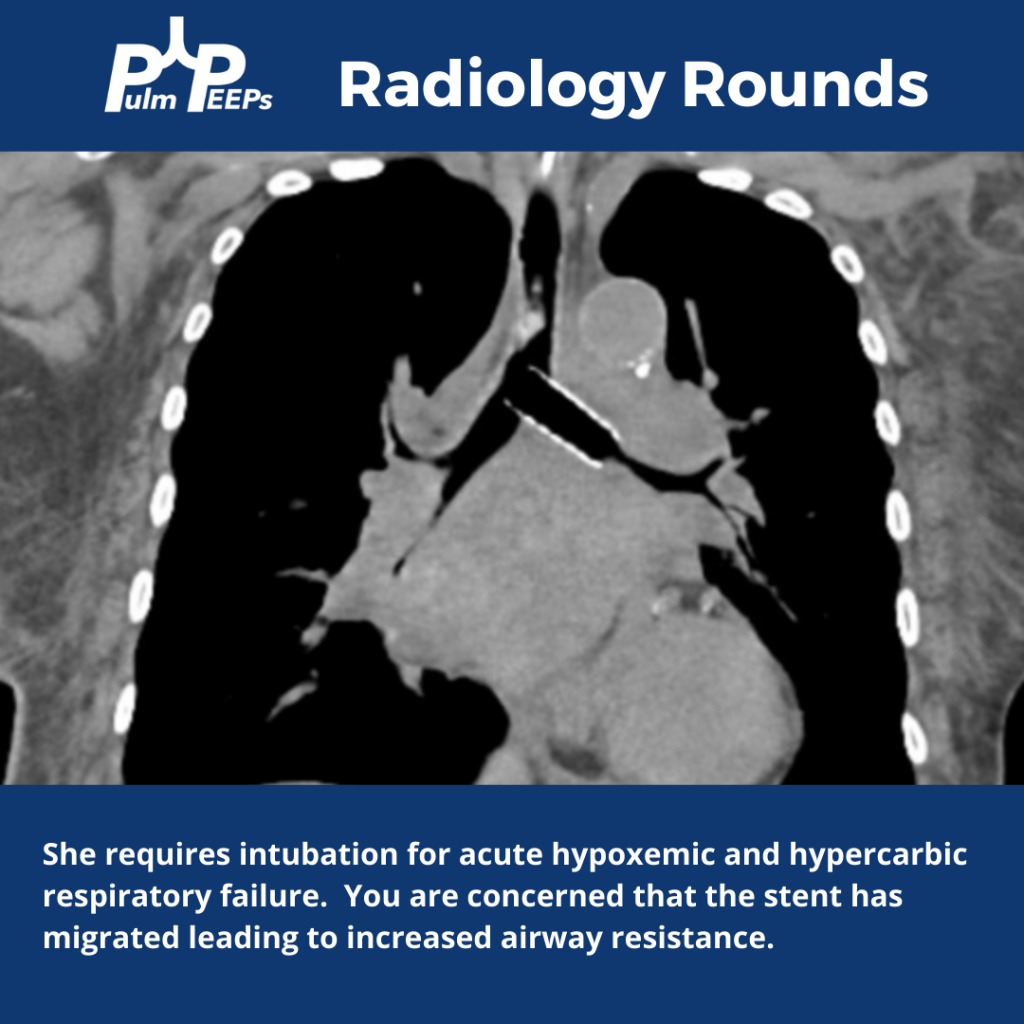
The patient is diagnosed with small cell lung cancer and requires a left bronchial stent. She develops acute hypoxemic and hypercapnic respiratory failure requiring intubation.
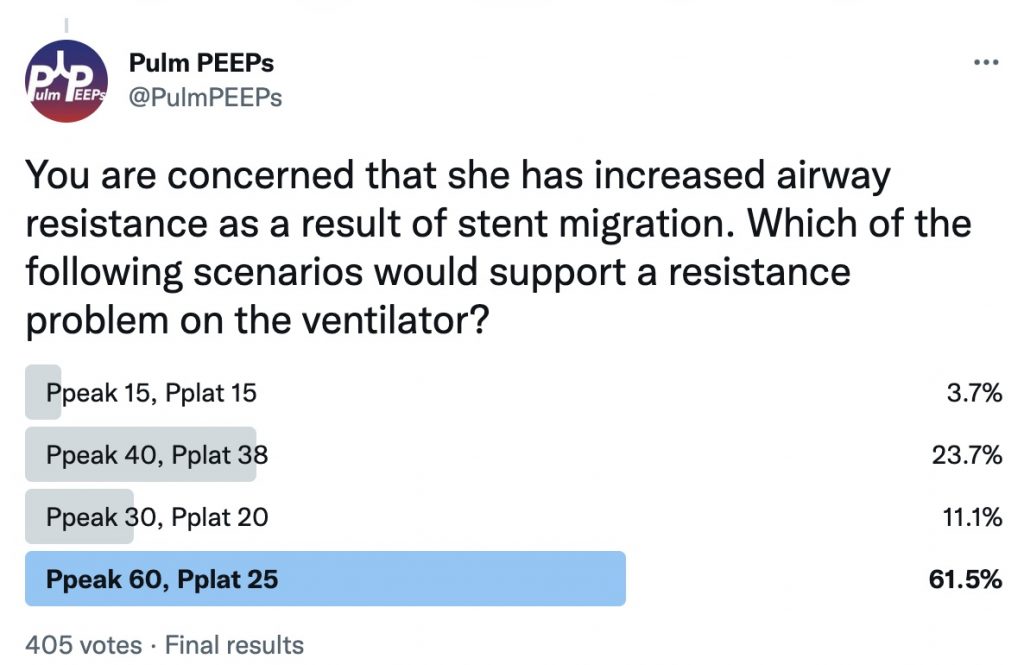
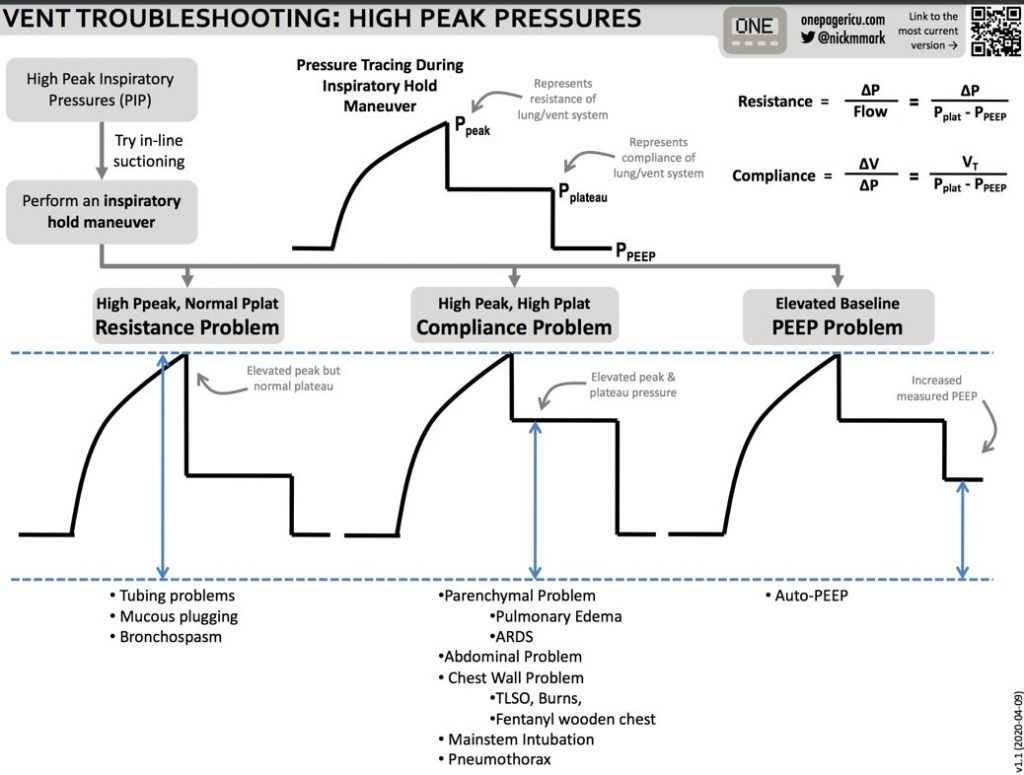
You are concerned that she has increased airway resistance as a result of stent migration. What would you expect to see on the ventilator if this is the case?
Here are some tips from ICU OnePager on interpreting high peak pressures on the ventilator