We’re back with our second episode in our guideline initiative, and continuing our review of the Global Initiative for Asthma (GINA) guidelines on asthma. In our first episode of this series, we talked about making the diagnosis of asthma, the importance of appropriate phenotyping, and doing an initial assessment of asthma severity. Today, we’re discussing the initial management of asthma and discussing but pharmacologic and non-pharmacologic treatments. We have a great infographic prepared along with the episode, and a boards-style question for your review.
Meet Our Co-Hosts
Rupali Sood grew up in Las Vegas, Nevada and made her way over to Baltimore for medical school at Johns Hopkins. She then completed her internal medicine residency training at Massachusetts General Hospital before returning back to Johns Hopkins, where she is currently a second year pulmonary and critical care medicine fellow alongside Tom. Rupali’s interests include interstitial lung disease, particularly as related to oncologic drugs. And she also loves bedside medical education.
Tom Di Vitantonio is originally from New Jersey and attended medical school at Rutgers, New Jersey Medical School in Newark. He then completed his internal medicine residency at Weill Cornell, where he also served as a chief resident. He currently is a second year pulmonary and critical care medicine fellow at Johns Hopkins, and he’s passionate about caring for critically ill patients, how we approach the management of pulmonary embolism, and also about medical education of trainees to help them be more confident and patient centered in the care they have going forward.
Key Learning Points
- Introduction to Asthma Guidelines
- The podcast continues a guideline series on asthma, focusing on the Global Initiative for Asthma (GINA) 2024 guidelines.
- Emphasizes practical applications for clinicians managing asthma in different settings.
- Importance of Evidence-Based Asthma Management
- Asthma treatment must be systematic and personalized, considering recent clinical evidence.
- Previous reliance on short-acting beta agonists (SABAs) as rescue inhalers has shifted towards inhaled corticosteroid (ICS)-containing therapies.
- Over-reliance on SABAs is linked to increased exacerbations, airway inflammation, and poor long-term outcomes.
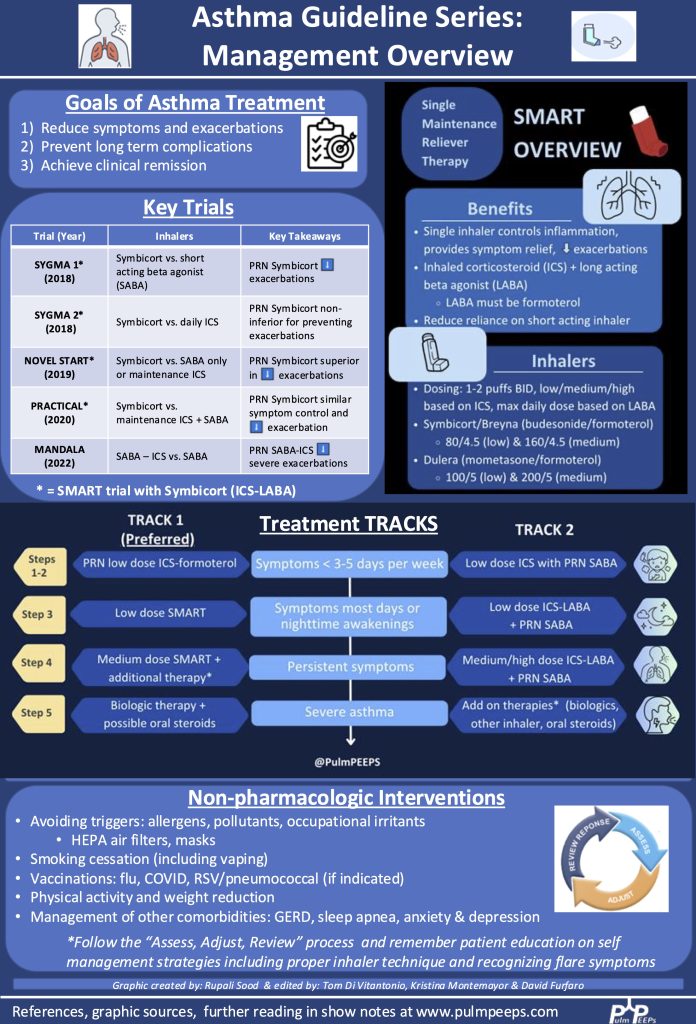
- Stepwise Approach to Asthma Management (GINA 2024)
- The Track 1 approach (preferred) centers around ICS-formoterol as both maintenance and reliever therapy (MART).
- Track 2 (alternative approach) includes daily ICS or ICS-LABA with a separate SABA as a reliever.
Stepwise Therapy
- Step 1-2 (Mild asthma): Low-dose ICS-formoterol as needed for symptom relief.
- Step 3 (Moderate asthma): Low-dose maintenance ICS-formoterol (MART therapy).
- Step 4 (Persistent symptoms): Medium-dose ICS-formoterol (MART) with additional inhaler adjustments.
- Step 5 (Severe asthma): Consider biologic therapies, phenotyping, and additional controllers.
- MART Therapy as a Game-Changer
- Maintenance and Reliever Therapy (MART):
- Uses a single inhaler for both daily maintenance and symptom relief.
- Reduces overuse of SABAs.
- Provides real-time up-titration of ICS during exacerbations.
- Leads to better adherence and control.
- Supporting Evidence from Trials:
- SIGMA 1 & 2, Novel Start, Practical (2018-2019): Showed ICS-formoterol reduces exacerbations and steroid exposure compared to SABAs.
- MANDALA (2022): Showed ICS-SABA improves outcomes over SABA alone, though not a true MART study.
- Practical Considerations in Asthma Management
- Patient adherence is critical—educate on proper inhaler use and symptom monitoring.
- Insurance and cost barriers may require prescribing alternative inhalers.
- Review and adjust treatment regularly using the “Assess, Adjust, Review” framework.
- Avoid high-dose ICS without exploring additional controller therapies like LAMAs, leukotriene receptor antagonists (Montelukast), and azithromycin.
- Non-Pharmacologic Interventions
- Smoking cessation (including vaping/marijuana).
- Weight management and physical activity.
- Avoiding triggers (allergens, occupational exposures, pollution).
- Air purifiers and HEPA filters.
- Vaccinations (flu, COVID-19) to prevent viral exacerbations.
- Managing comorbidities (GERD, sleep apnea, anxiety/depression).
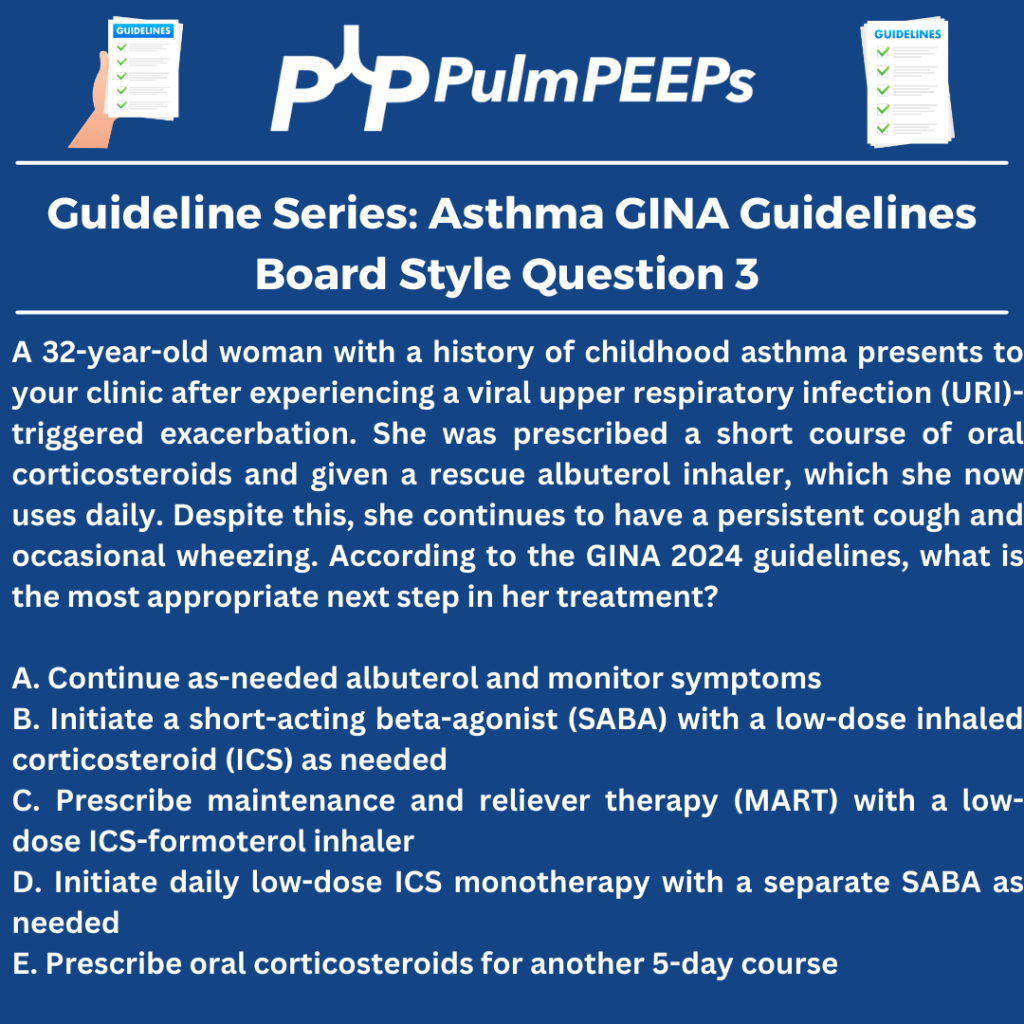
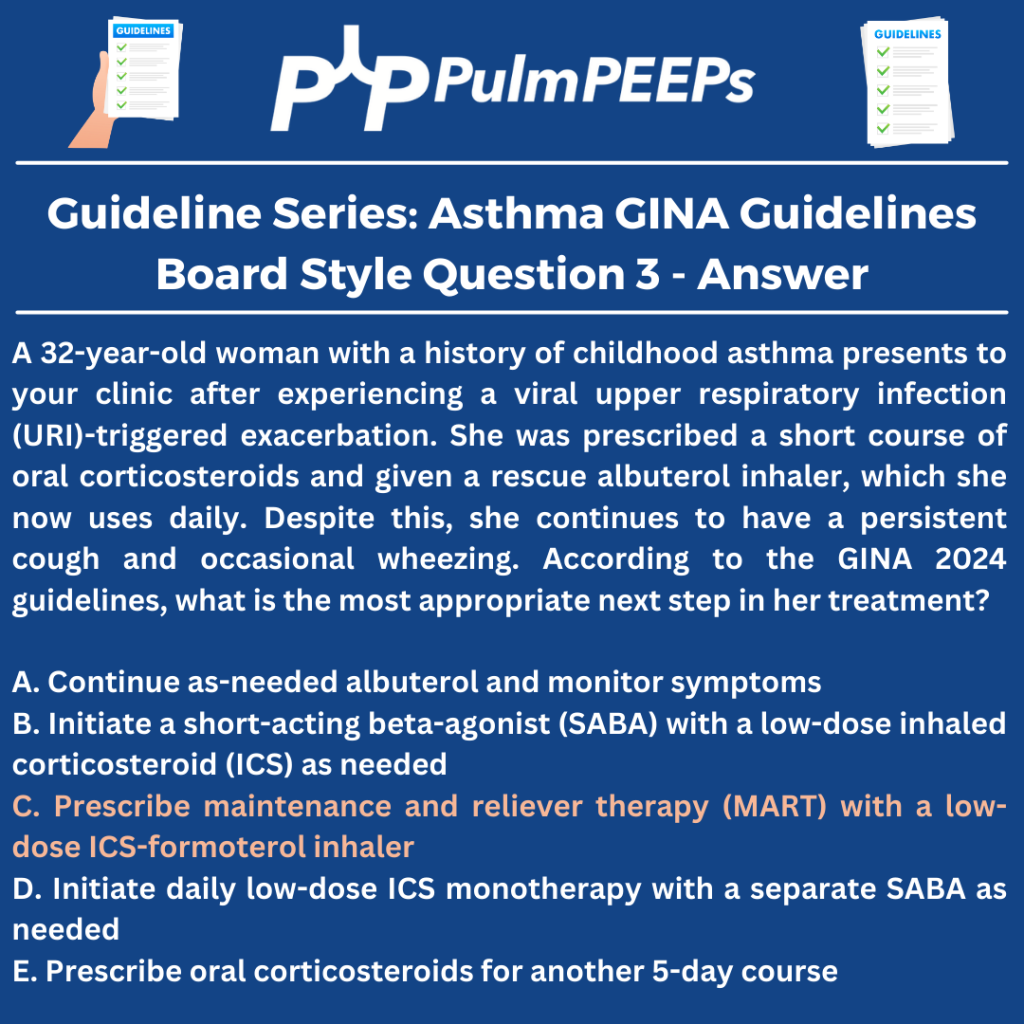
- Case Discussion & Real-World Application
- Patient with recurrent asthma symptoms post-viral illness.
- Started on low-dose ICS-formoterol as needed.
- Symptoms persisted, leading to maintenance ICS-formoterol (MART therapy).
- Regular follow-up to monitor and adjust therapy.
- Looking Ahead
- Next episode will focus on biologic therapies for severe asthma.
- Emphasis on ongoing education, practical application, and patient-centered care.
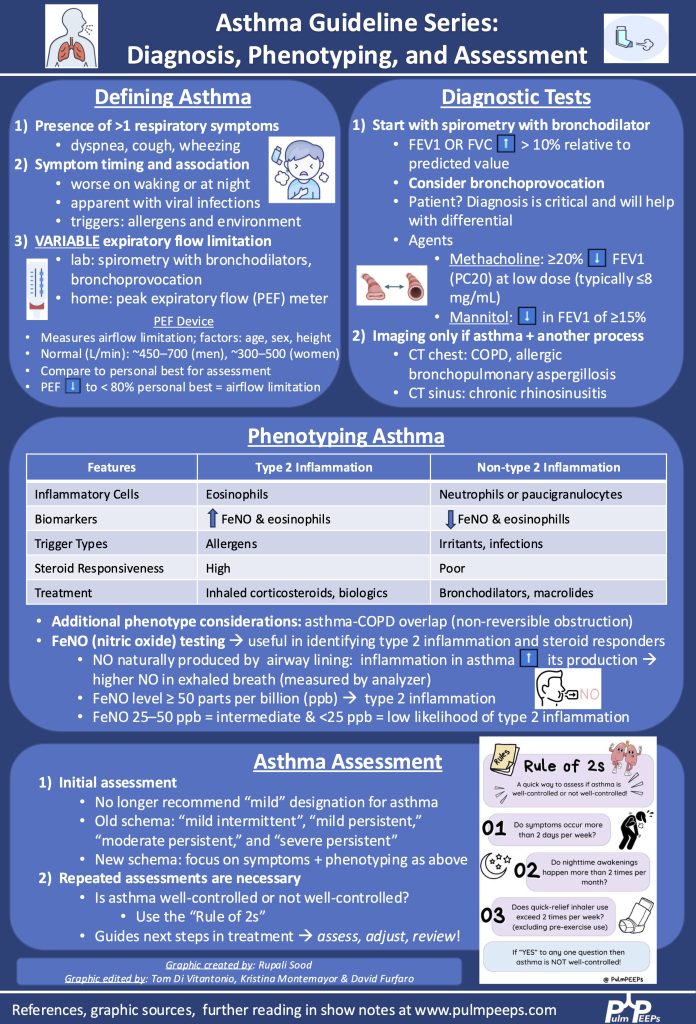
Infographic
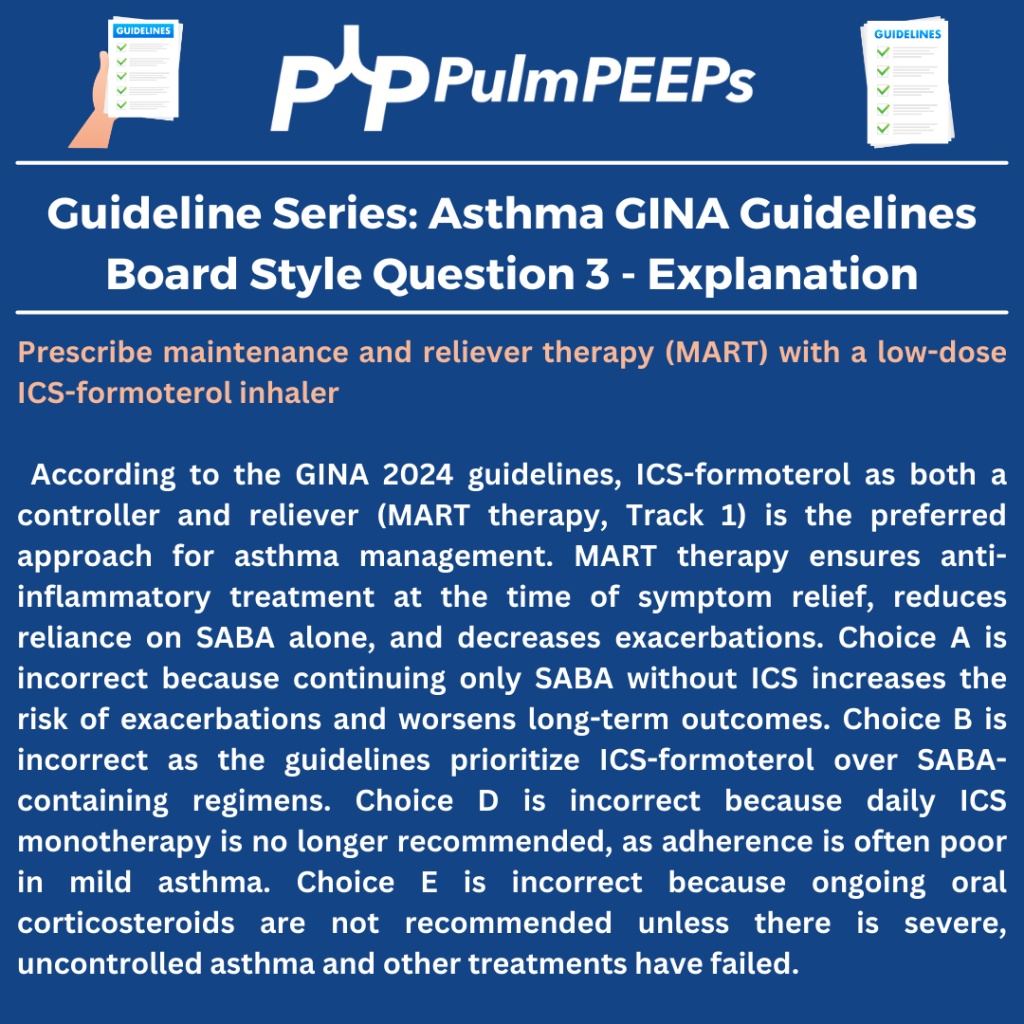
Boards Style Question
References
http://ginasthma.org/2023-gina-main-report/
https://www.uptodate.com/contents/an-overview-of-asthma-management-in-children-and-adults
https://onlinelibrary.wiley.com/doi/full/10.1111%2Fresp.14782
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS | More