We are thrilled today to be previewing CHEST 2023! The Annual Meeting is taking place October 8th – 11th in Honolulu, Hawaii, and we are joined today by CHEST enthusiasts and the past, present, and future conference chairs. Listen now to hear what is in store for you next month in Hawaii, to plan your conference experience, and find out what sessions are can’t-miss!
Meet Our Guests
Aneesa Das is a Professor of Medicine at The Ohio State University Wexner Medical Center. She is the Assistant Director of the OSU Sleep Program and the Director of the Portable Sleep Testing Program. She was the Vice-Chair of the CHEST 2022 Scientific Programming Committee, and the Chair for 2023
Subani Chandra is an Associate Professor at Columbia University. She is the Vice Chair of Medicine for Education, and the internal medicine residency program director. She was the chair of the CHEST Scientific Program Committee for CHEST in 2022 and joined us when we came to you live from Nashville last year. Subani is currently the Chair for the Training and Transitions Committee for CHEST.
Gabe Bosslet is a Professor of Clinical Medicine in the Department of Pulmonary, Critical Care, Sleep and Occupational Medicine at Indiana University. He is the Assistant Dean for Faculty Affairs and Professional Development at IU. He is the current Vice Chair of the CHEST 2023 Scientific Programming Committee and the Chair Elect for CHEST 2024.
Huzaifah Salat is a budding clinician educator who is currently working as a consultant pulmonologist and intensivist at Advocate Aurora Health in Wisconsin. He recently completed his Pulmonary and Critical Care Fellowship at the University of Oklahoma Health Sciences Center. He has worked with Pulm PEEPs before on some fantastic Tweetorials.
CHEST’s Local Efforts and Initiatives to Support Survivors of the Maui Wildfires
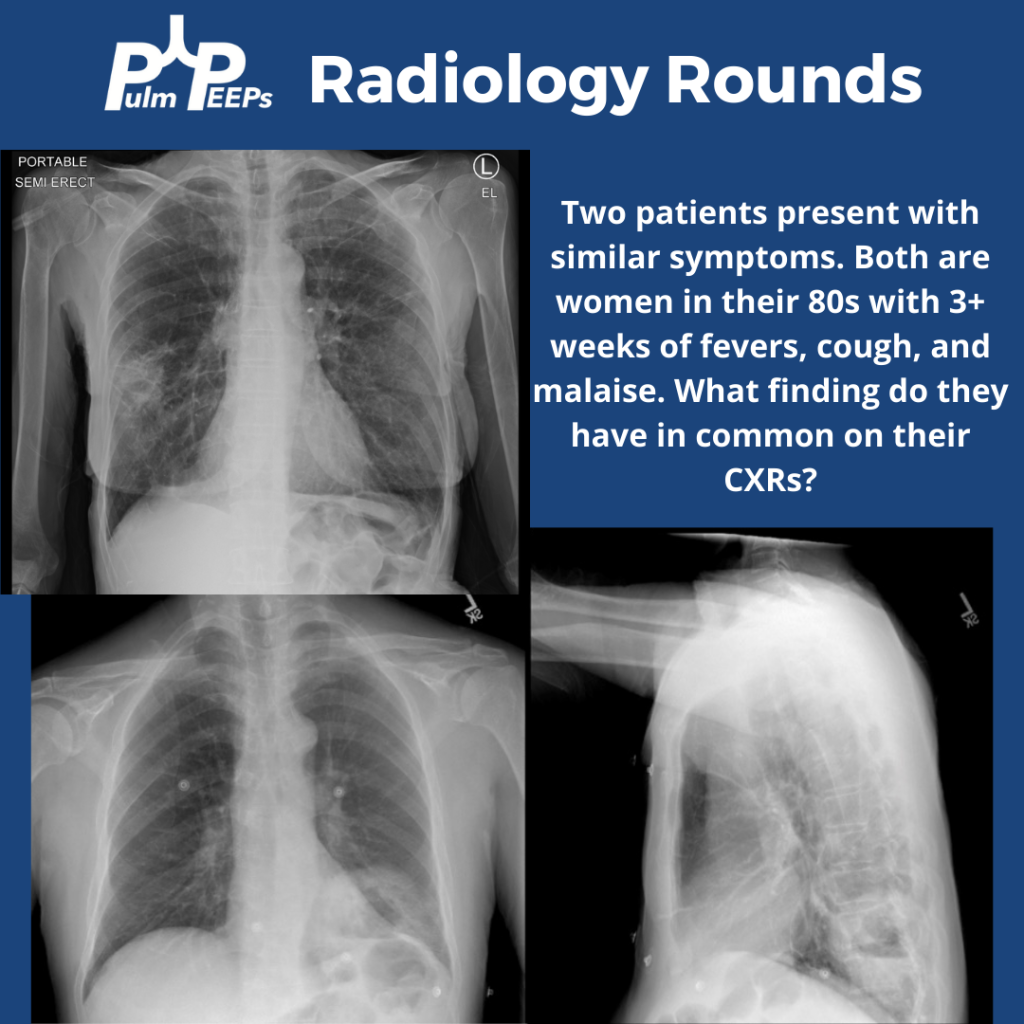
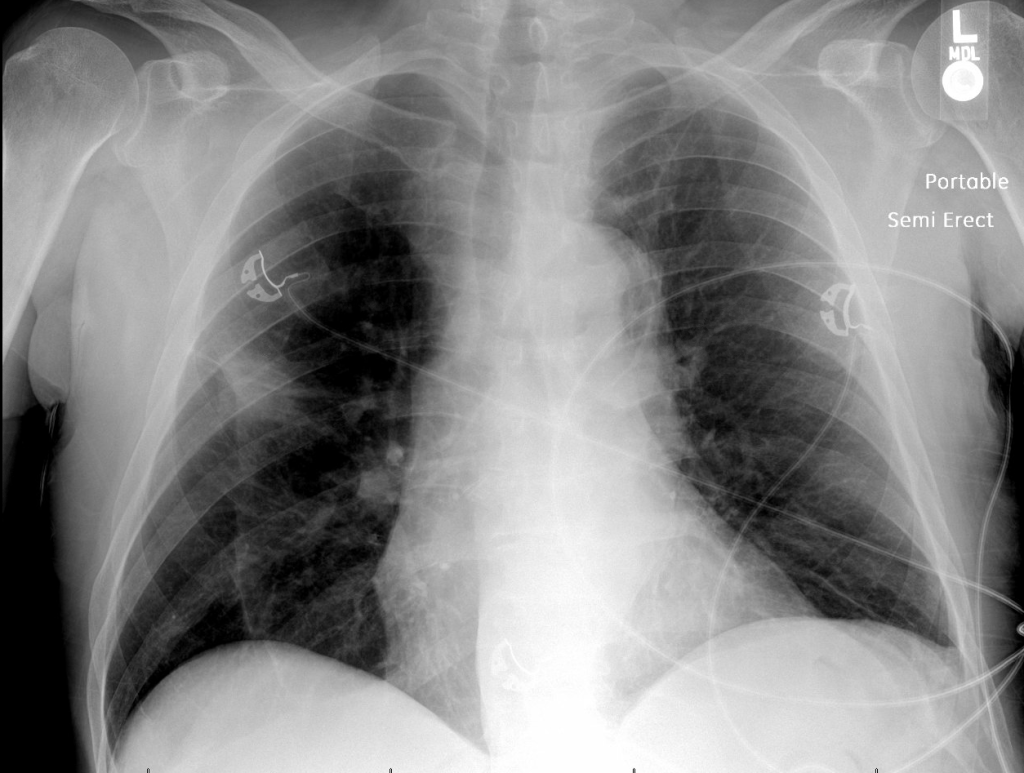
Tuesday is time for another #RadiologyRounds! Time for some CXR reading and a differential diagnosis mnemonic Two women presented to the hospital with similar presentations. They are both in their 80s with multiple weeks of cough, fever, and fatigue. Here are the CXRs
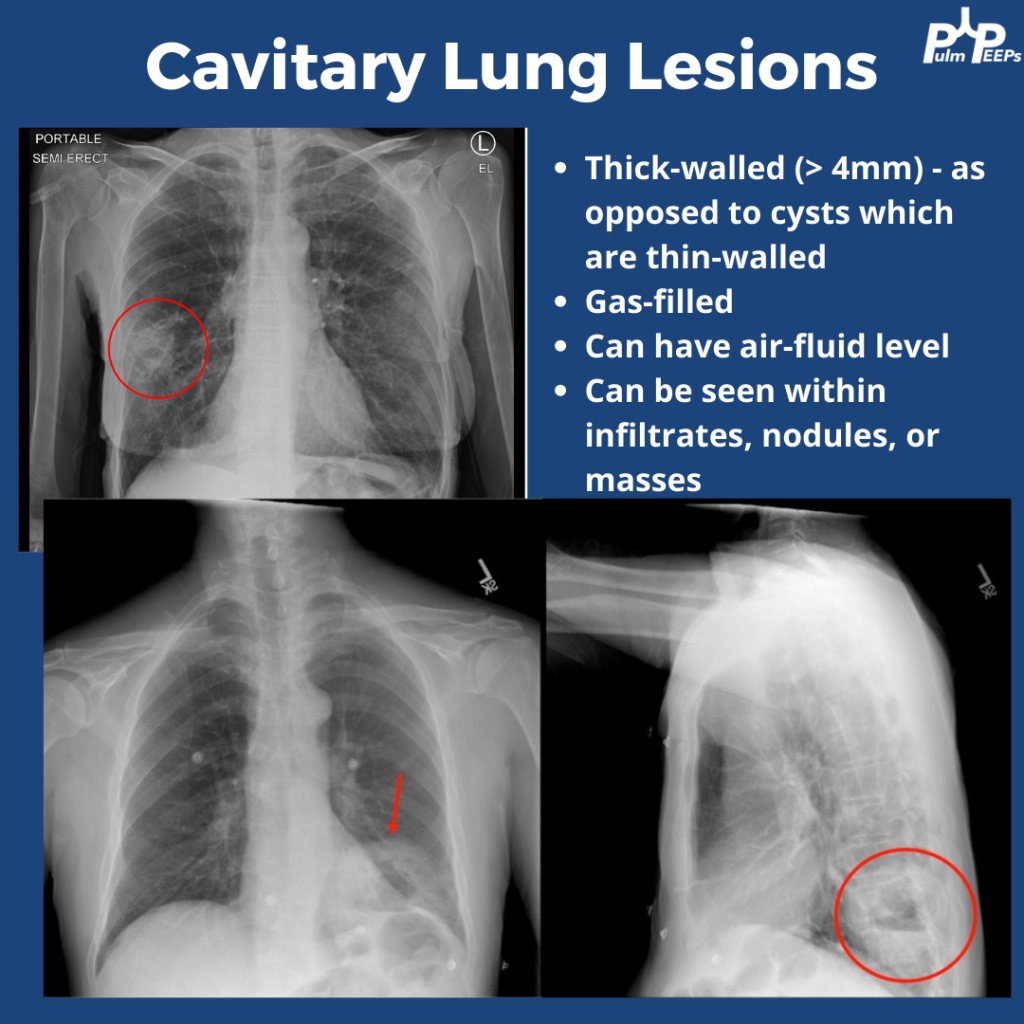
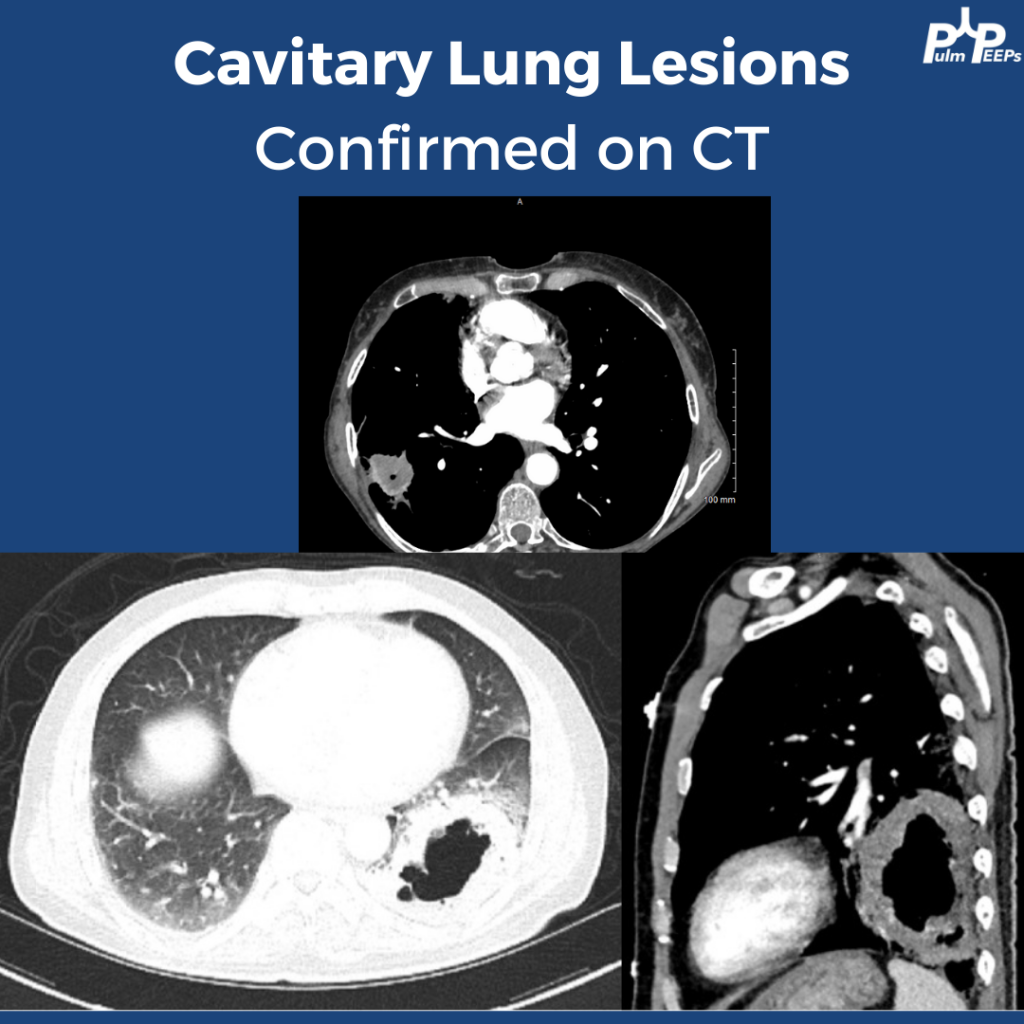
The CXRs both showed cavities. They are thick-walled (>4mm) and gas-filled. Cavitary lung lesions are seen within infiltrates, nodules, or masses. There can be an air-fluid level within the cavity. Cysts have thinner walls. The findings were confirmed on CT scan
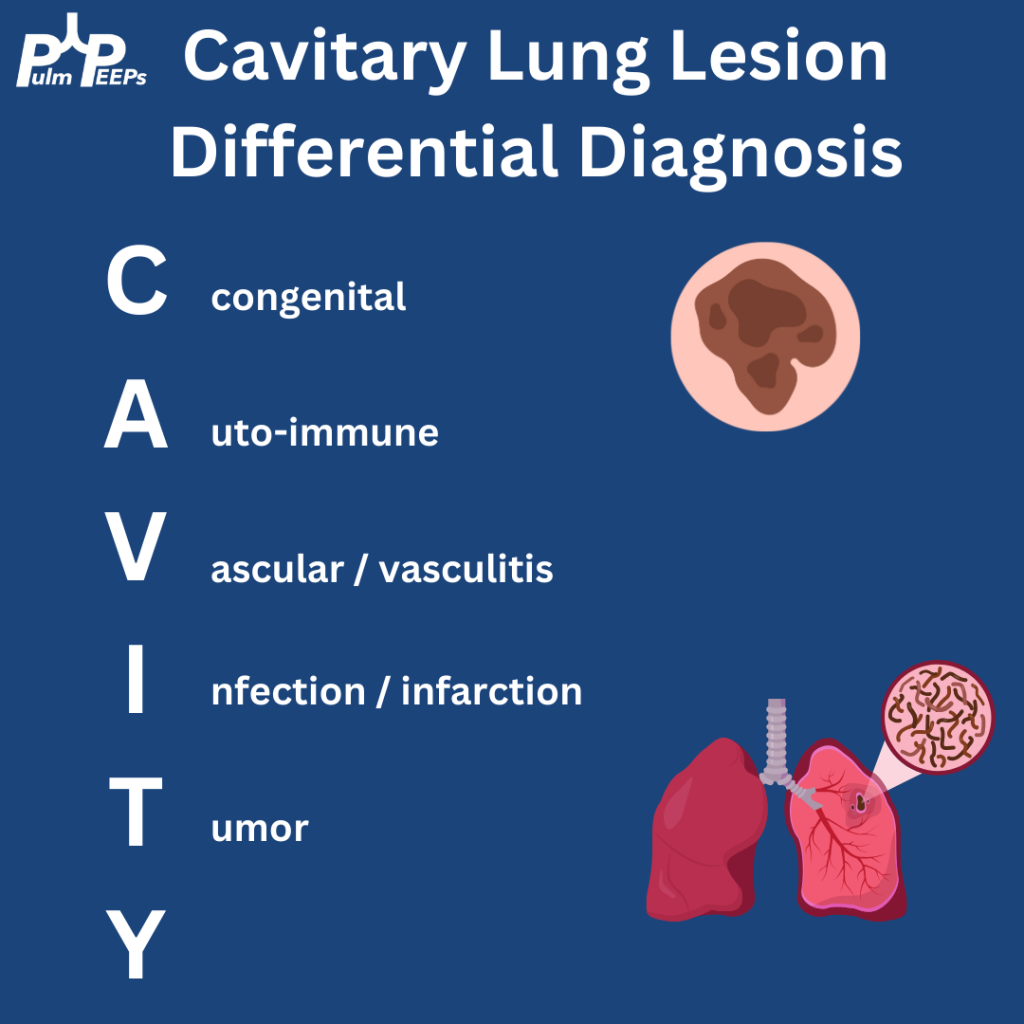
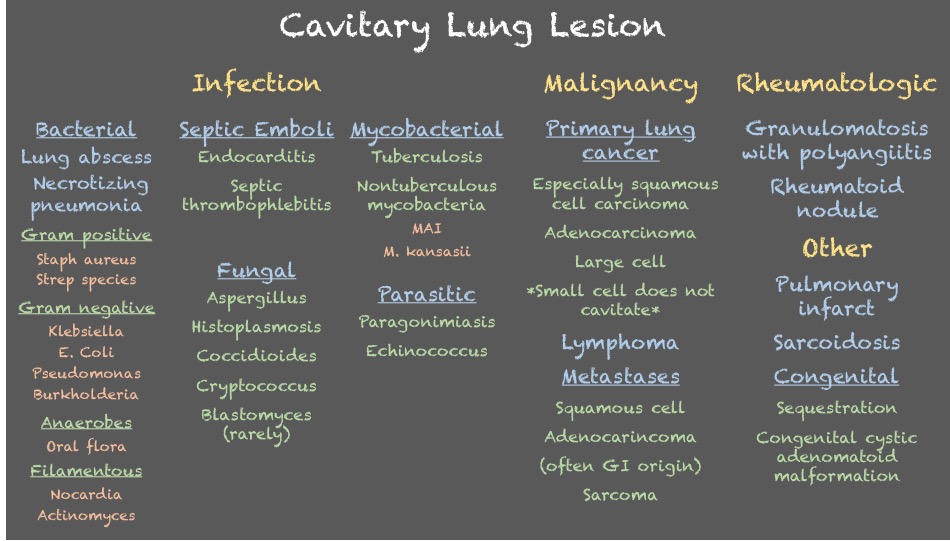
Cavitary lung lesions can have a broad differential so it is helpful to have a systematic approach. To make it easy, when you see this just remember: CAVITY
Bonus points to anyone who can fill in the Y
Both patients were ultimately diagnosed with pulmonary abscesses which improved with prolonged courses of antibiotics with anaerobic and gram-negative coverage.
We’re excited to be back with another Fellows’ Case Files. Today, we’re visiting the University of Pittsburgh to meet a fantastic fellow and a dedicated educator, and to hear about a fascinating case. Let us know if you’ve ever had a similar case, and share your interesting cases with us!
Meet Our Guests
Rachel Wojcik obtained her B.S. in Biology from Mercyhurst University and a Master’s in Liberal Studies from the University of Denver in Global Affairs with a focus on Healthcare. She completed her MD at the University of Colorado before completing her residency and chief resident year at the University of Pittsburgh and has continued her training at Pitt for PCCM fellowship.
Dr. Stephanie Maximous is an Assistant Professor of Medicine at the University of Pittsburgh School of Medicine and is the Clinical Education APD for the Pulmonary and Critical Care Fellowship program. She completed her fellowship at Pitt in addition to obtaining a Master’s Degree in Medical Education there. She teaches in and directs courses throughout the medical school, residency, and fellowship and was recently awarded the 2023 Outstanding Subspecialty Teaching Attending Award from the housestaff.
Case Presentation
Patient: A 70-year-old male with a history of idiopathic thrombocytopenia on chronic prednisone and a history of tobacco use disorder.
Presentation: Came to the hospital with 2-3 days of right-sided weakness and slurred speech.
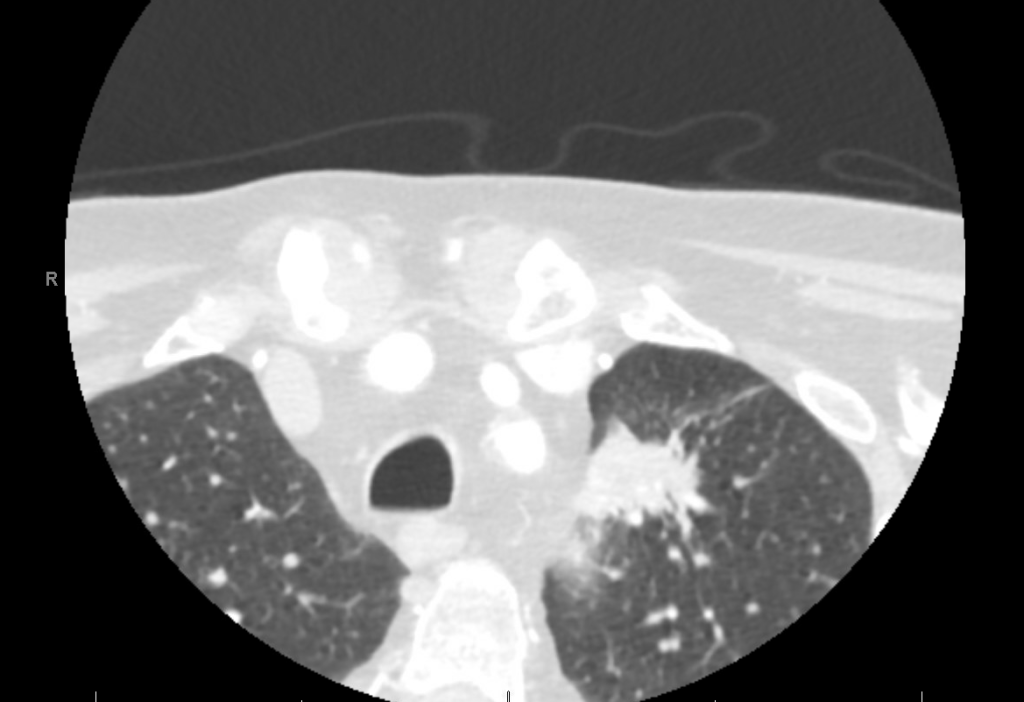
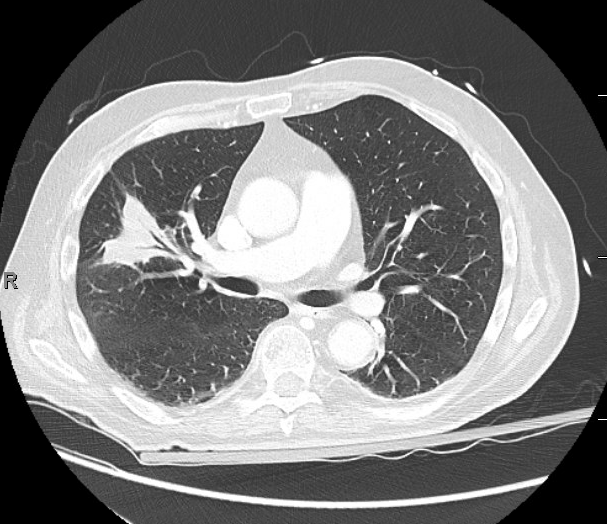
Findings: MRI showed a moderate-sized left pontine stroke. A CT angiogram of the neck showed no evidence of an occlusion, but a spiculated two-centimeter nodule at the apex of the left lung was found.
Additional Information: He requires a walker for mobility and needs help with activities like taking a shower and dressing. He had an unintentional 20-pound weight loss over six months, increased fatigue, and malaise.
Previous Investigations: A chest x-ray ordered two months prior by his hematologist was unremarkable, and a CT of the abdomen and pelvis showed no masses.
Key Learning Points
Bronchoscopy in Decision Making:
The decision to perform bronchoscopy in patients depends on a myriad of factors, including the location of any lesions, accessibility, potential risks, and the potential diagnostic yield.
Fiber optic bronchoscopy with BAL can rule out infections, and if no diagnosis is reached, more invasive methods like surgical biopsy might be necessary.
Consider the location of consolidated masses; navigational bronchoscopy might be needed for lesions without a clear airway leading into them.
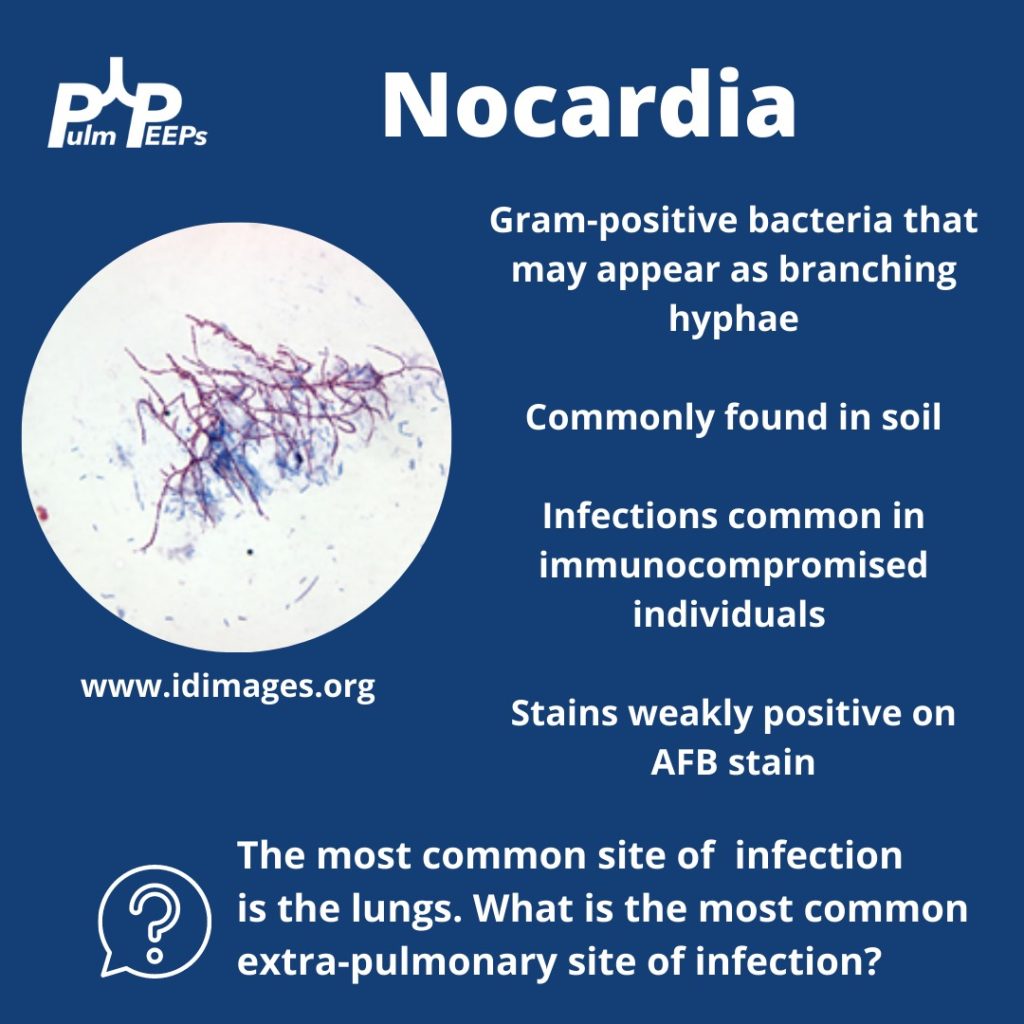
Nocardia Insights:
Nocardia is a gram-positive bacterium that stains weakly acid-fast.
It can be found in soil and certain water sources and can infect through the skin or by inhalation.
Two-thirds of patients with Nocardia are immunocompromised.
The dosage of Bactrim given for PJP prophylaxis doesn’t prevent Nocardia infections in immunocompromised individuals.
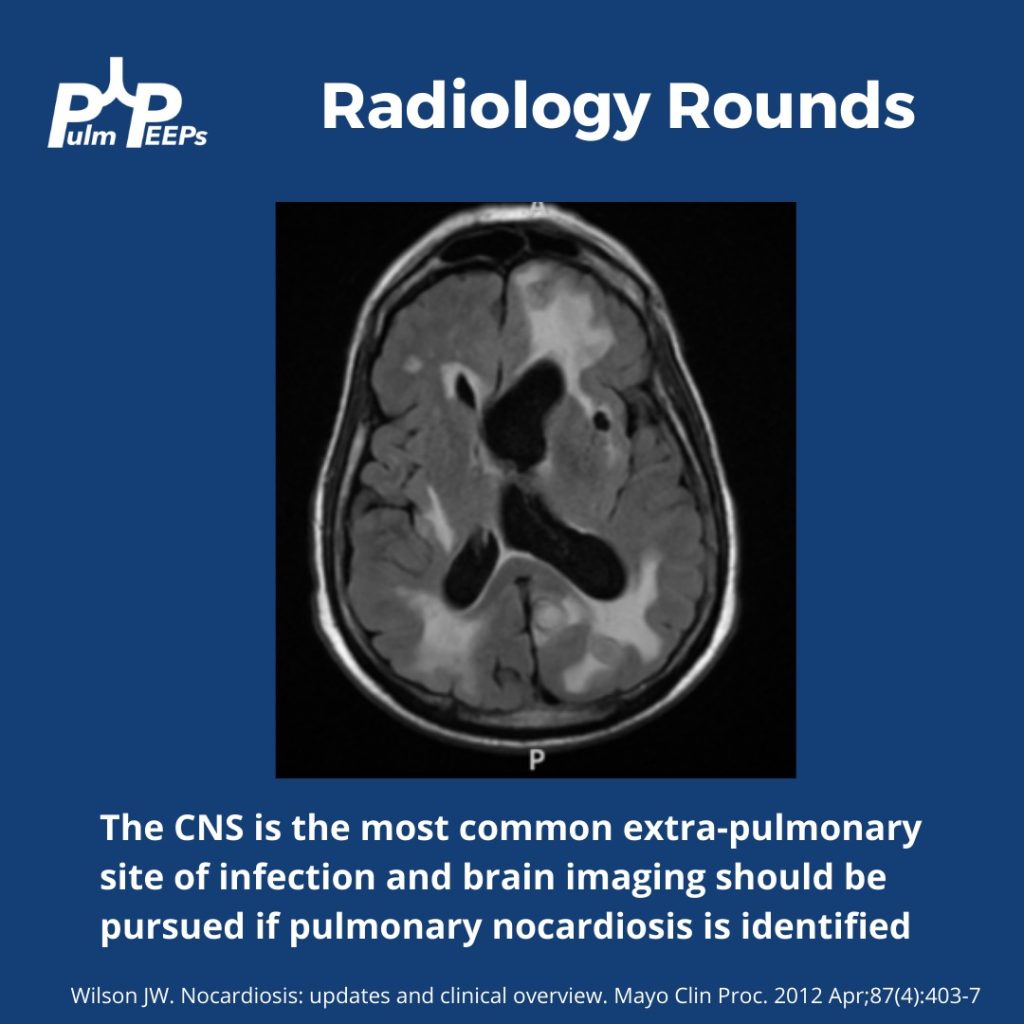
While the lungs are the most common infection site, Nocardia can manifest elsewhere, like the skin or CNS.
Treatment Approach:
Bactrim is the mainstay of treatment for Nocardia. If someone is allergic, desensitizing them can be crucial.
IV induction phases vary in length depending on the severity of the disease.
The overall treatment duration is protracted to prevent relapse.
Takeaway Points:
Bactrim for PJP prophylaxis doesn’t necessarily prevent Nocardia infections in immunocompromised individuals.
If someone is allergic to Bactrim, consider desensitizing them due to its importance in treating Nocardia.
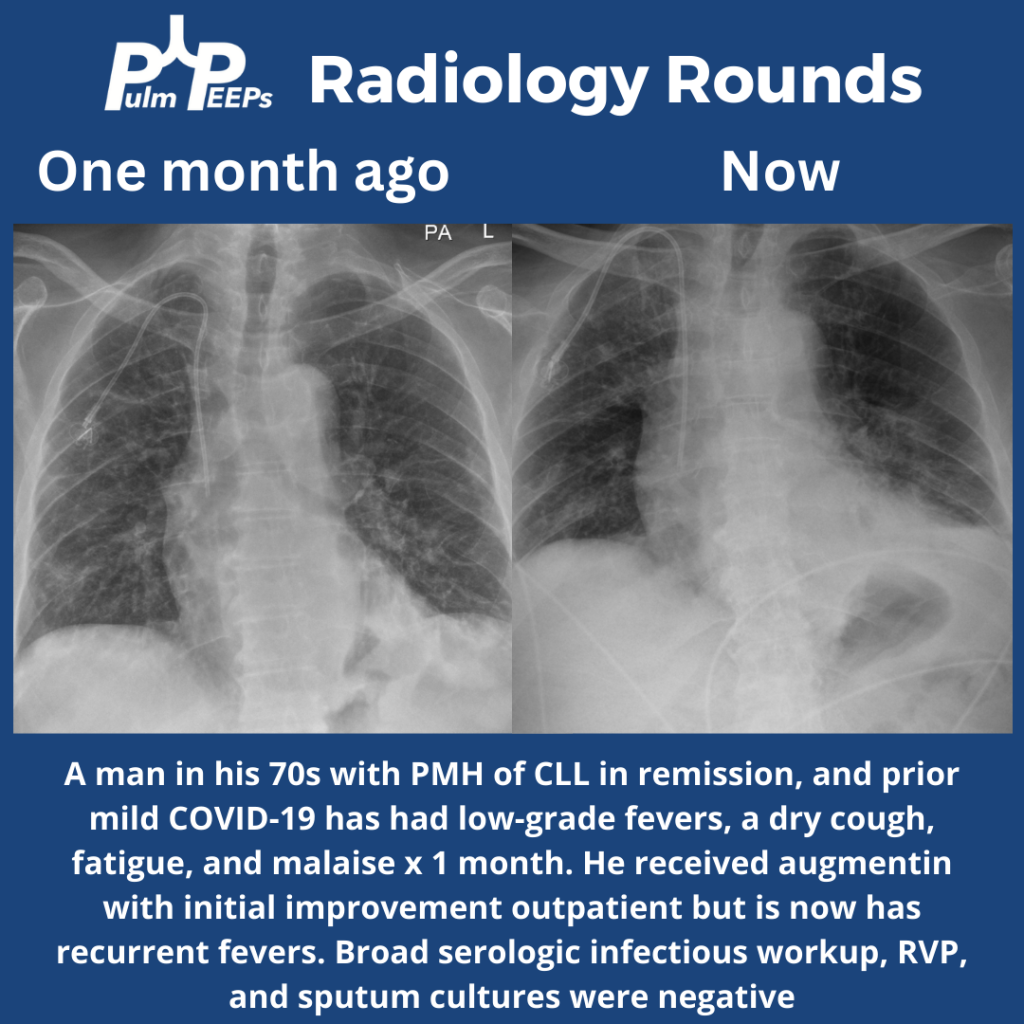
Time for #RadiologyRounds! This week we have a man in his 70s with CLL s/p treatment now in remission. He had fevers, a dry cough, and malaise that initially improved outpatient with antibiotics but have now recurred.
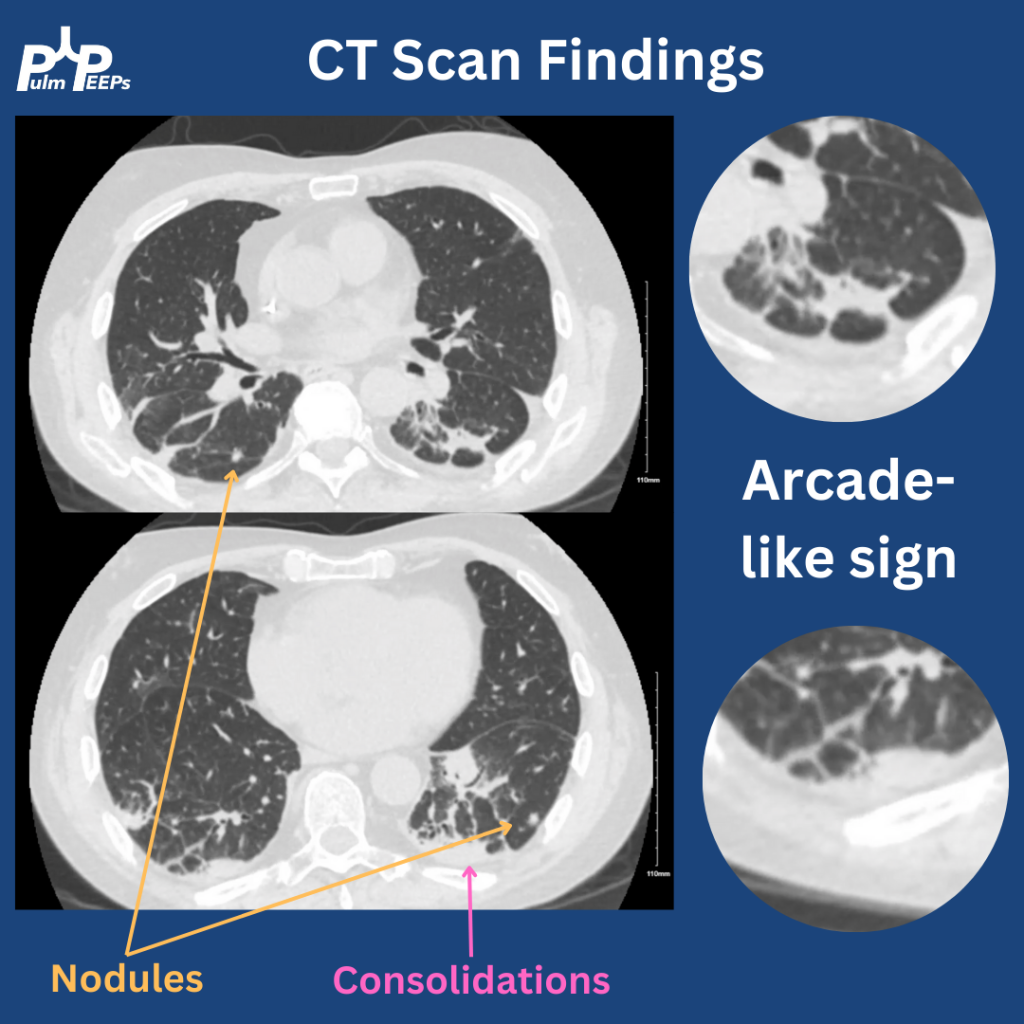
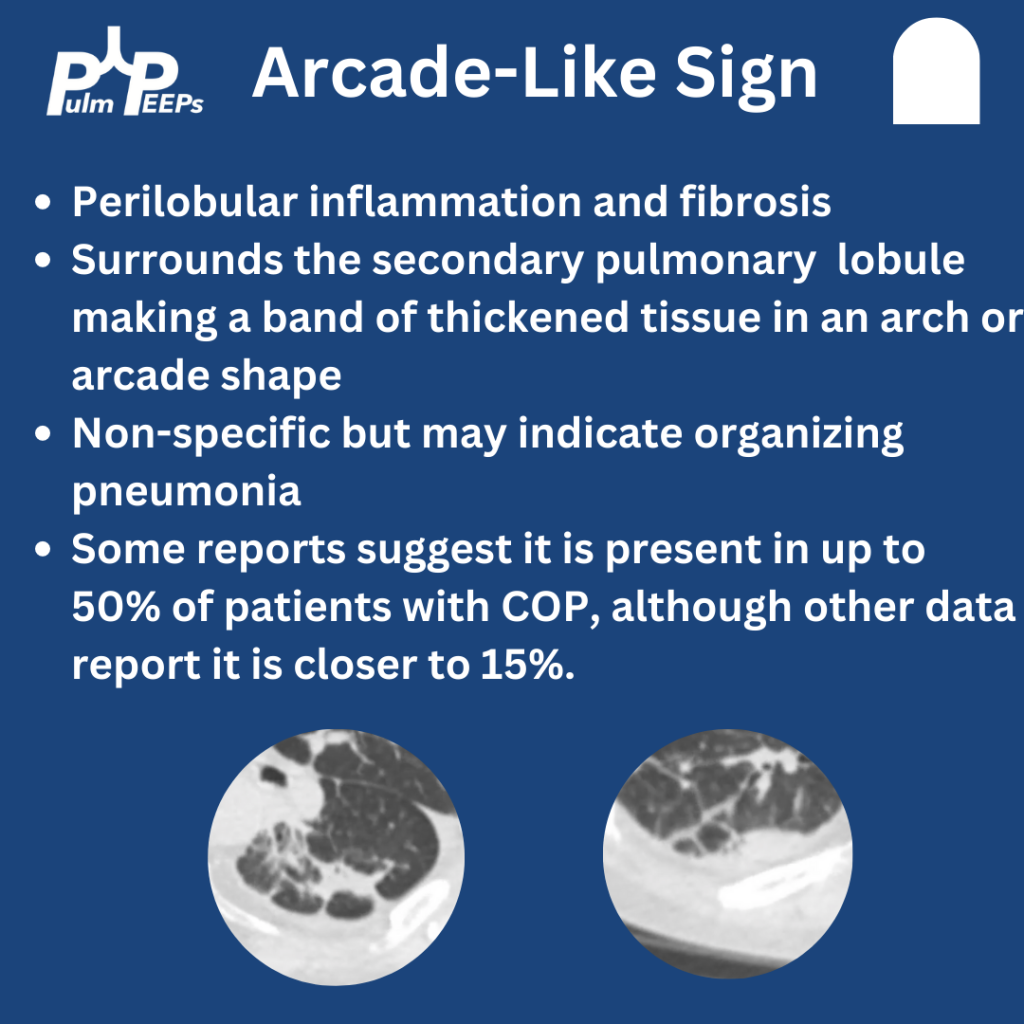
The CT had multiple findings including small nodules, consolidations, and bands of fibrosis around the secondary pulmonary nodules. This is known as Arcade-Like Sign and has classically been described with COP. While it can make you think COP, it has a low sensitivity
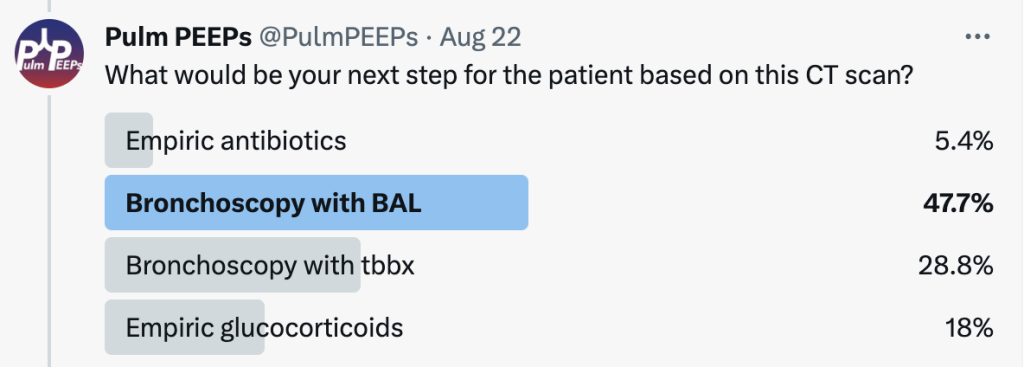
The patient underwent bronchoscopy with Tbbx given the suspicion for OP. The BAL was negative for bacterial, viral, fungal, or mycobacterial infection. The histopathology revealed organizing pneumonia. The patient was started on glucocorticoids and all symptoms improved
Welcome to our final episode highlighting content featured through the ATS Critical Care Assembly from ATS 2023. Today we are going to be talking about one of the Critical Care Assembly symposiums entitled: Fail Smarter and Learn Faster: Moving Beyond Bystander Training to Organizational Strategies to Reinforce the DEI Pipeline in Pulmonary and Critical Care Medicine.
Meet our Guest
Liz Viglianti is an Assistant Professor of Medicine at the University of Michigan. In addition to obtaining her MD at Duke, and completing her residency and fellowship at Michigan, she also has an MPH and completed a Masters of Science in Health and Healthcare Research at the University of Michigan. Her research focuses include persistent critical illness and sexual harassment within medicine.
Juan Celedón is a Professor of Pediatrics, and a Professor of Medicine, Epidemiology, and Human Genetics at the University of Pittsburgh, where he is also the Division Chief of Pediatric Pulmonology. In addition to his MD and pulmonary pediatric specialty, he has a doctoral degree in Public Health. He is a world renowned researcher, has been recognized for his scientific achievements by multiple societies including the ATS and the American Pediatric Society, leads large NIH funded research initiatives, and is the author of 100s of publications.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
Time for another Radiology Round by our Associate Editor Tess Litchman!
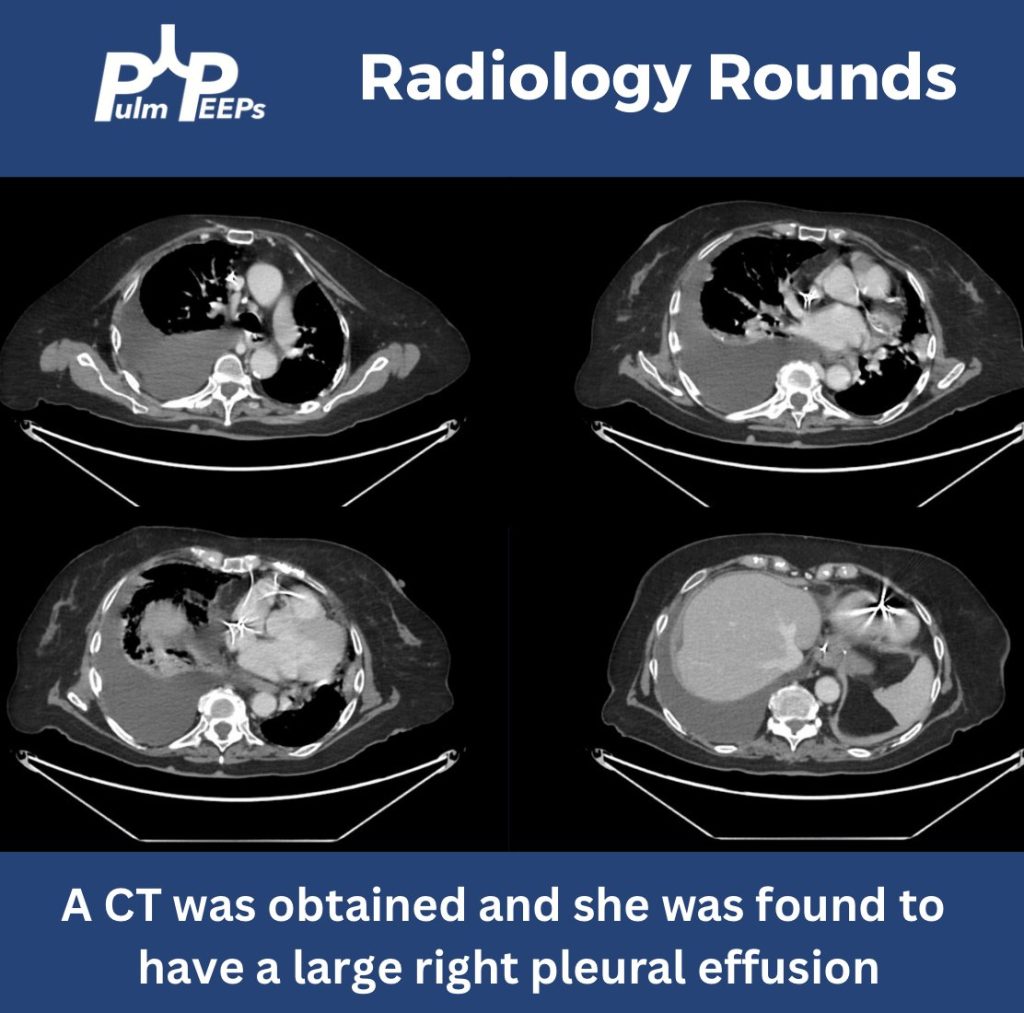
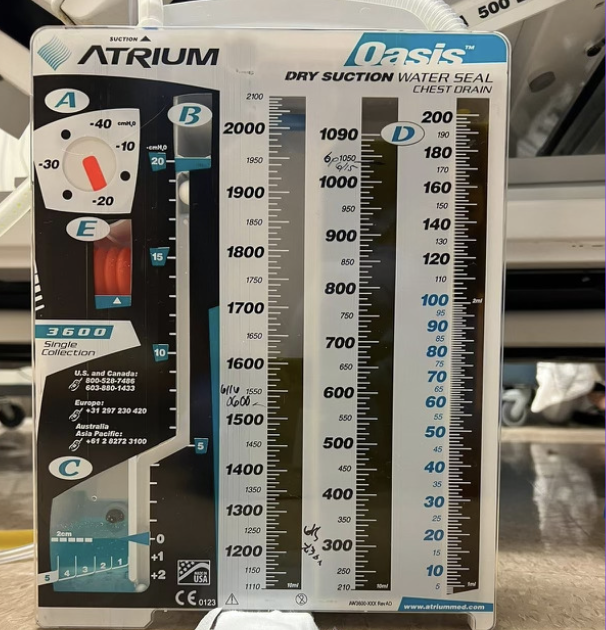
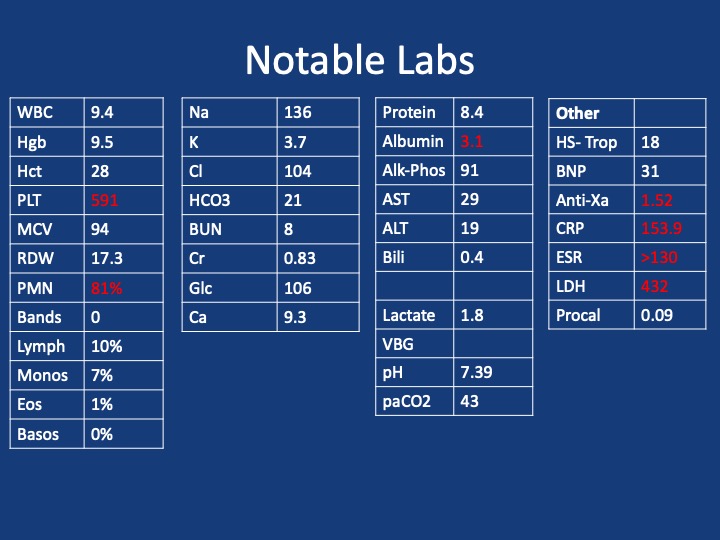
We have an older-aged woman found to have gastric and duodenal ulcers requiring multiple abdominal surgeries and transhepatic biliary drainage presenting with respiratory distress
She underwent pleural fluid drainage with the following pleural fluid studies
She ultimately had a right chest tube placed with 1.6 liters of green pleural fluid was drained
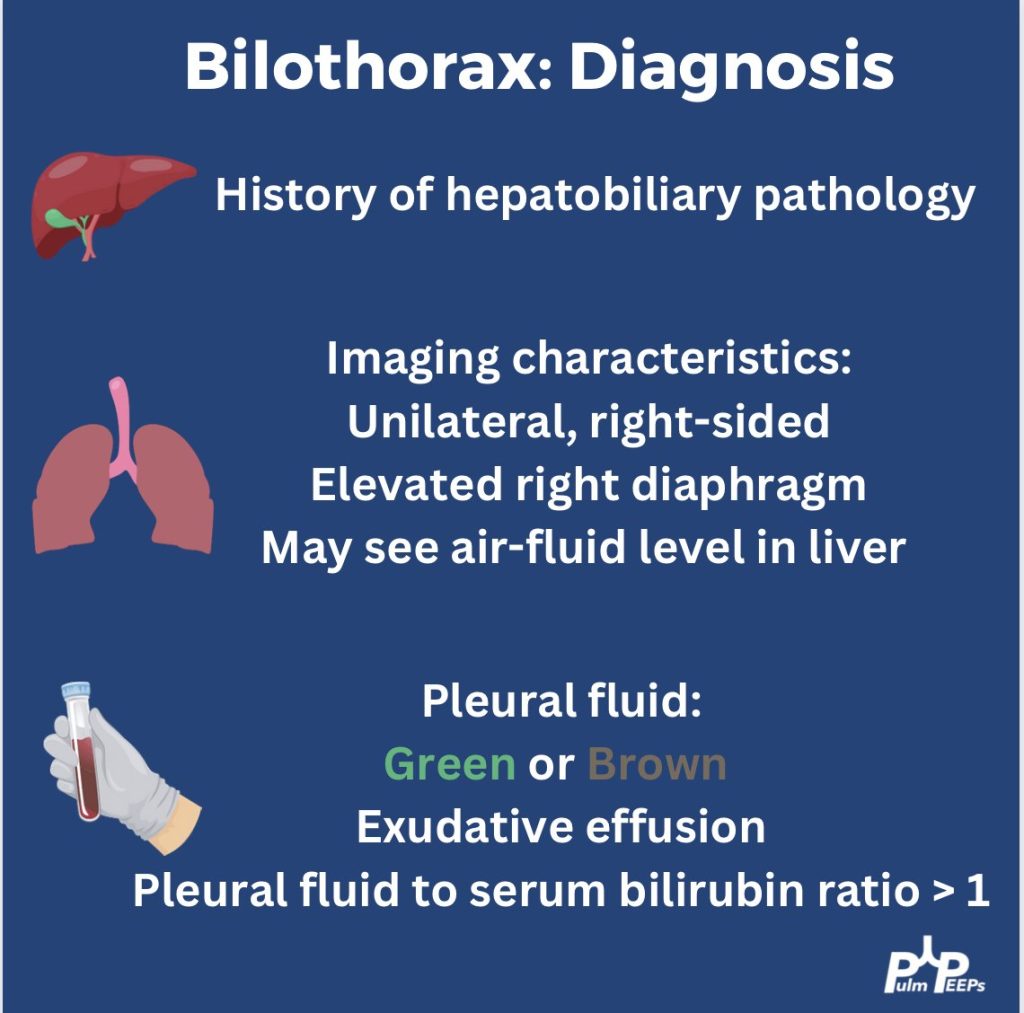
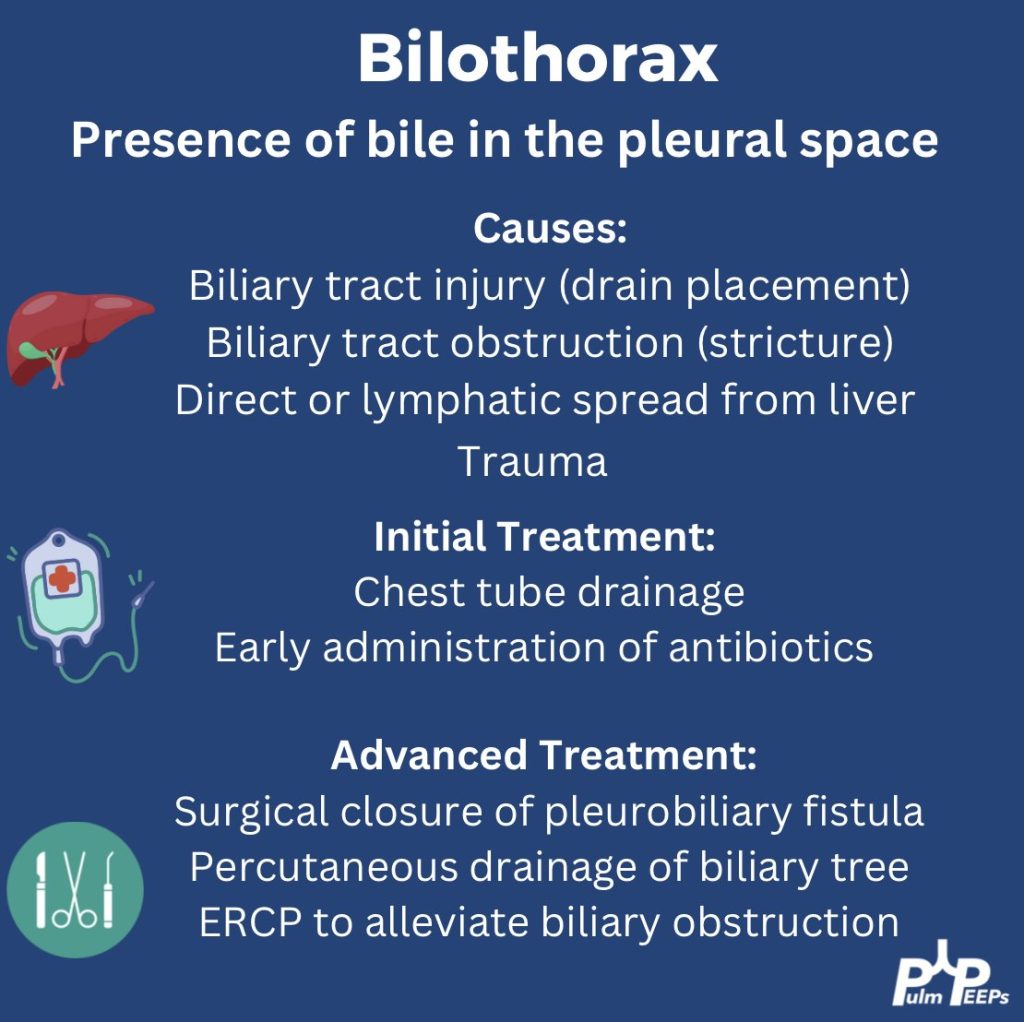
Given concern for a bilothorax, a pleural and serum bilirubin test were added. Her pleural bilirubin level was 17.2 and her serum bilirubin level was 0.5. Her chest tube was maintained, IV antibiotics were started and multi-disciplinary meetings occurred to determine next steps.
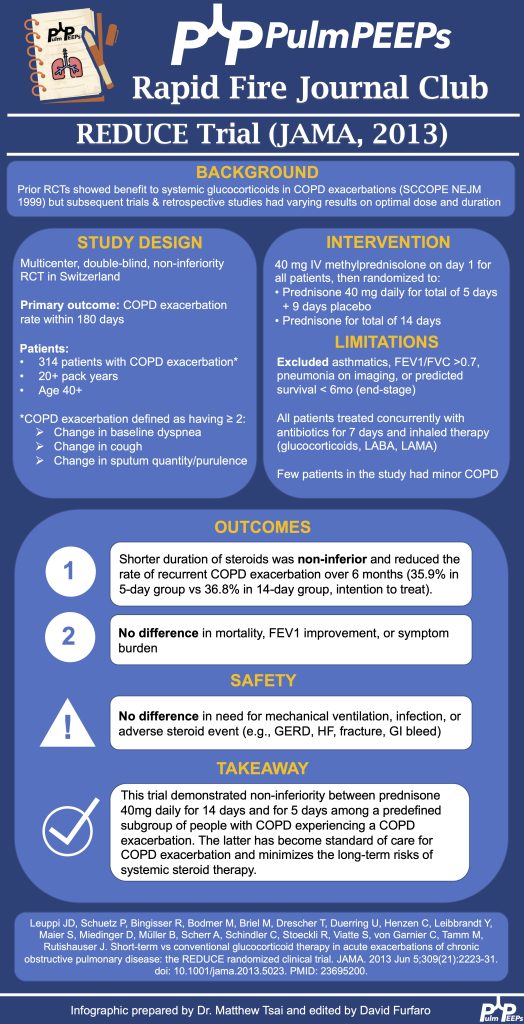
We’re back with our second episode of our Rapid Fire Journal Club. As a reminder, we will be reviewing articles in 10 minutes or less and sharing them with an infographic describing the findings of the trial. We are focusing on pulmonary trials to start.
Article and Reference
Today we’re talking about the 2013 REDUCE Trial in JAMA.
We’re diving back into some pleural fluid today (okay that is kind of gross to think about and we apologize). If you haven’t listened to our prior pleural effusion episodes and want to start from the top, then check out Episode 36 for a general approach to pleural effusions, and Episode 37 to hear about parapneumonic effusions. Malignant effusions are another common consult question and we’ll talk about everything from detection to monitoring, to definitive management.
Meet Our Guests
Dr. David DiBardino is an Assistant Professor of Medicine at the University of Pennsylvania Medicine and is the Associate Director for Clinical Research within the Section of Interventional Pulmonology. He is also the Program Director for the Interventional Pulmonary Fellowship there.
Dr. Jamie Bessich is an Assistant Professor of Medicine and Cardiothoracic Surgery at NYU Grossman School of Medicine. She is the Section Chief of Interventional Pulmonology and is the Director of Bronchoscopy at Tisch Hospital.
Dr. Van Holden is an Associate Professor of Medicine at the University of Maryland School of Medicine and is the Pulmonary and Critical Care Fellowship Program Director there. She was last on the show for our very first Fellows’ Case Files when we discussed a fascinating case of pulmonary alveolar proteinosis.
Case Presentation
The page: 72M smoker, new effusion, concern for malignancy, tap?
Further history: 72 year old man with PMH of GOLD B COPD, tobacco use (55 pack years), HTN, HLD, and diabetes. He presented to the ED with progressive dyspnea and fatigue. He is on LAMA/LABA for his COPD, and he does not frequently have exacerbations. He has no increased sputum production or wheezing, but he has been feeling progressively fatigued and lethargic. H Over the past few weeks he has had more dyspnea on exertion, and now has it at rest too. It is a bit worse when he lies flat. He has had no weight gain or edema in his legs and has actually lost 10-15 pounds in the last 3 months. In the ED, he is newly requiring 3-4L NC, has decreased breath sounds on the right, and a CXR shows a large right-sided pleural effusion, as well as a large apical nodule with some spiculation, both of which are new from prior.
Key Learning Points
Causes of malignant pleural effusion
–Lung cancer is the most common in men
–Breast cancer is the most common cause in women
–Lung and breast cancer account for > 50% of all malignant pleural effusions
–Other less common causes are lymphoma, GU or GI tract cancer
–Remember to consider mesothelioma
Prognosis of MPE
–Malignant pleural effusion means the cancer is advanced and stage 4 by definition
–The average life expectancy after a diagnosis of MPE is 3-12 months, depending on the patient and the malignancy
Imaging and MPE
–Make sure to get a CT scan after drainage so no lesions are missed
–Ultrasound can be helpful to look for disruptions of the pleural line, loculated fluid, or pleural nodules
Pleural fluid analysis
–Make sure to send common labs (gram stain, culture, pH)
–Cell count is very important as most MPE are lymphocyte-predominant
–Triglycerides can be helpful as well (more on chylothorax in future episodes)
–Cytology is essential and makes the diagnosis. The sensitivity is 65 – 75 percent so repeat taps may be needed and you need to send at least 60 cc of fluid (often more)
–If you have high suspicion and no diagnosis after two taps, pleuroscopy and pleural biopsy is warranted
Management of MPE
–First you need to determine if the MPE is recurrent. This requires drainage and then monitoring
— The main options are repeat thoracenteses, pleurodesis, or indwelling pleural catheter. A combination can often be used, and shared decision making is essential to the determining the best option
–The three things to consider with recurrent malignant pleural effusion are:
Did the patient feel better after drainage?
Did the lung fully re-expand?
What is the best option for this specific patient to optimize quality of life and time outside of the hospital?
–In AMPLE, pleural cetehters and talc pleurodesis were compared, and both are reasonable options with equivalent outcomes on quality of life; although pleural catehters had fewer hospital days overall.
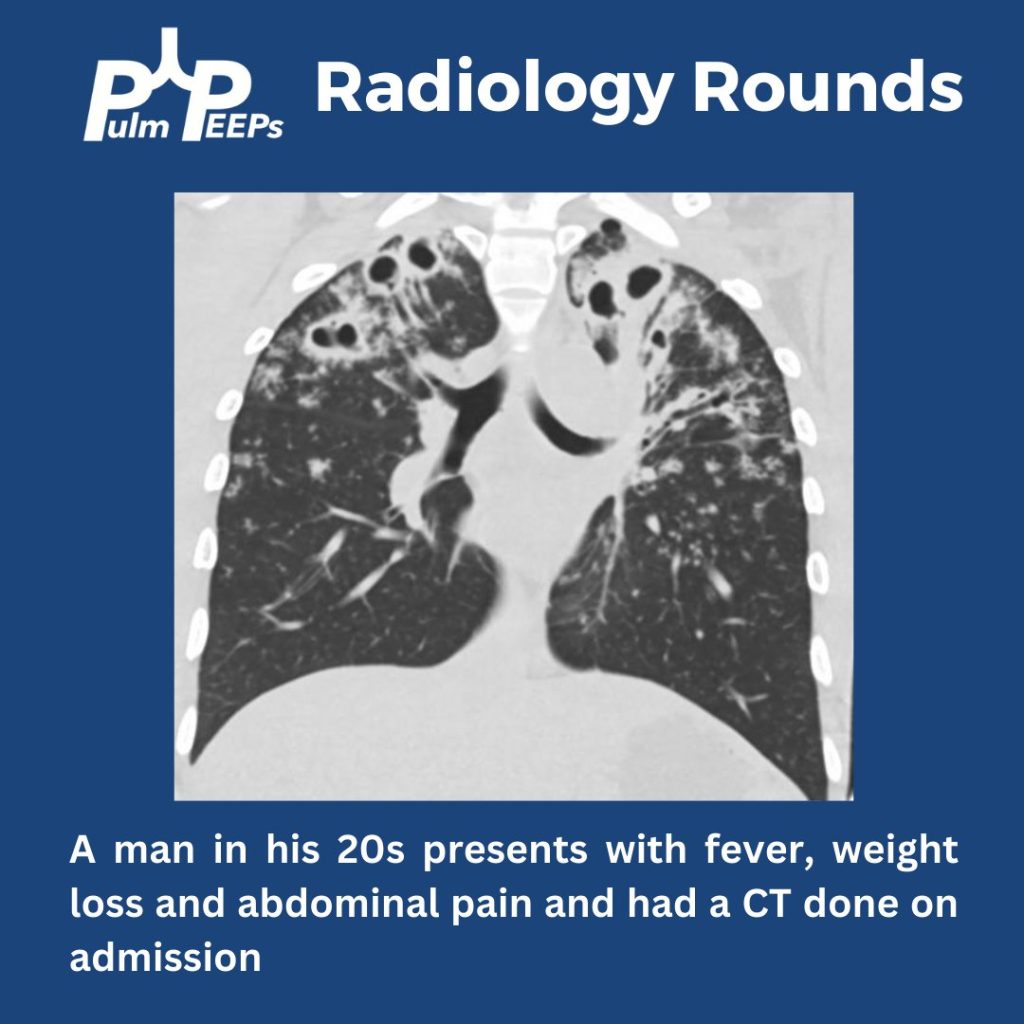
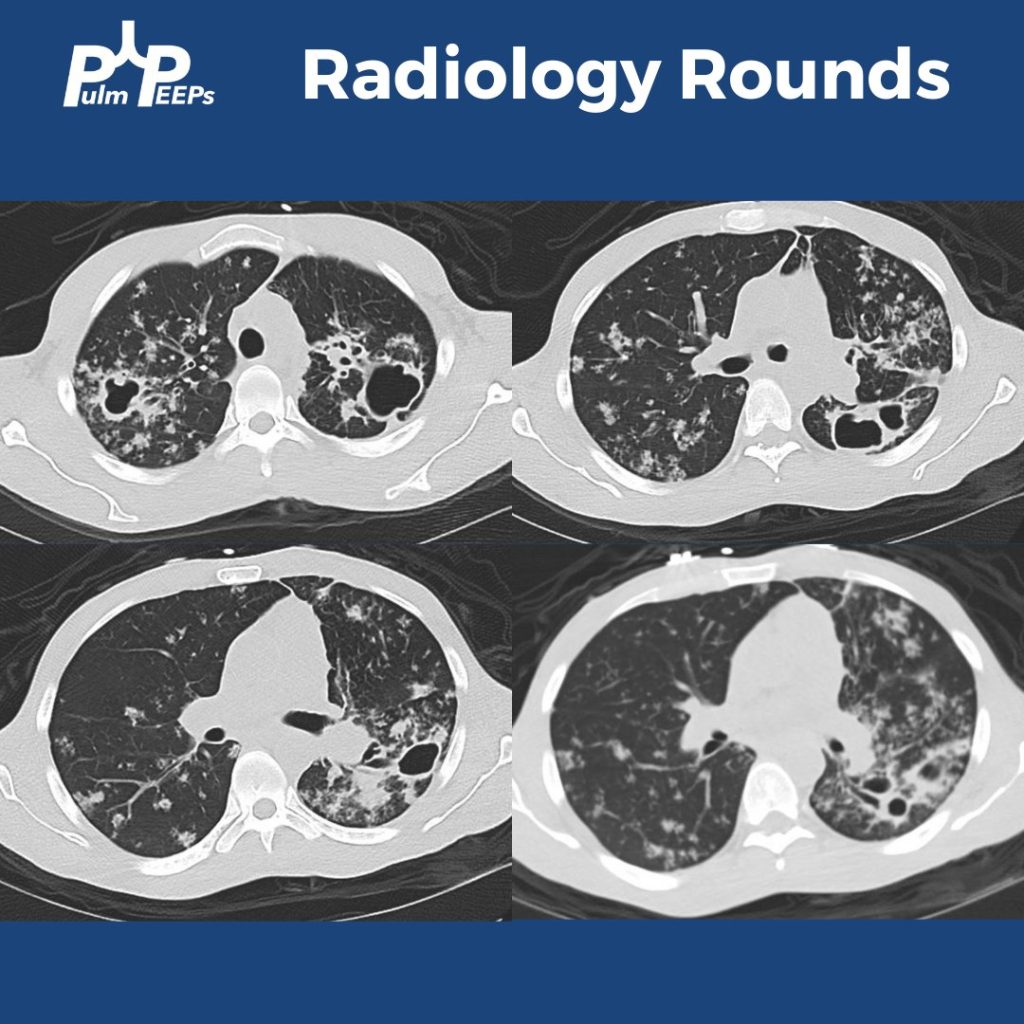
We are back with our first #RadiologyRounds of the new academic year. We have a young, immunocompetent man presenting with fever, weight loss, and abdominal pain.
What abnormalities are seen on his chest imaging?
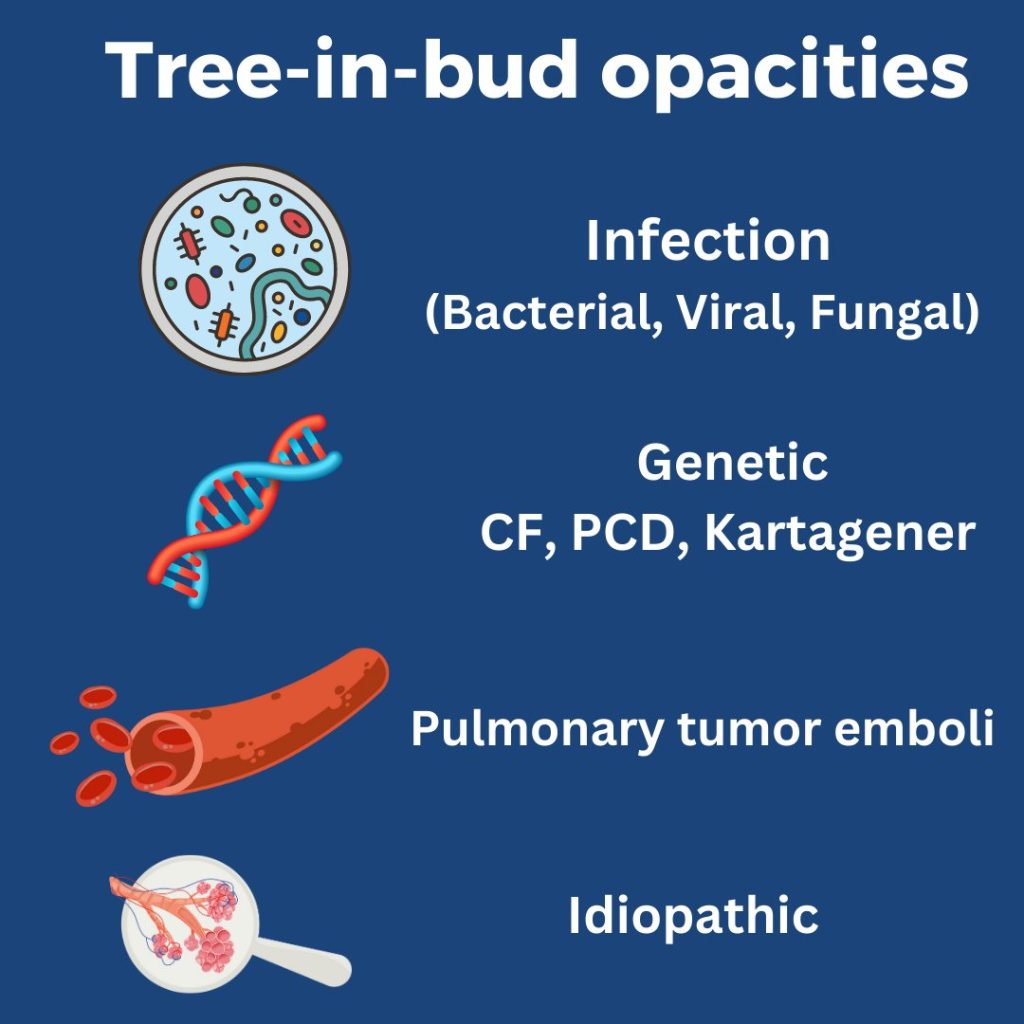
He was found to have bilateral apical cavitary disease, centrilobular nodules, and tree-in-bud opacities. He developed a productive cough with blood-tinged sputum as well as diarrhea.
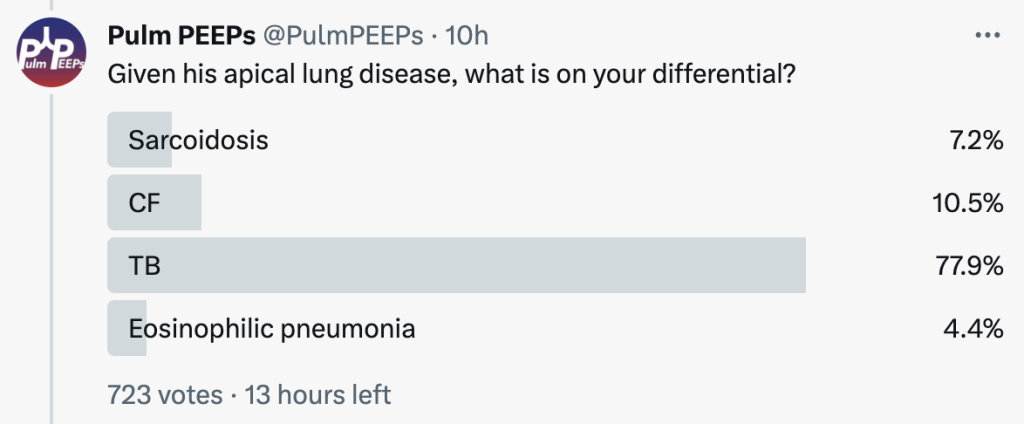
Given his apical lung disease, what is on your differential?
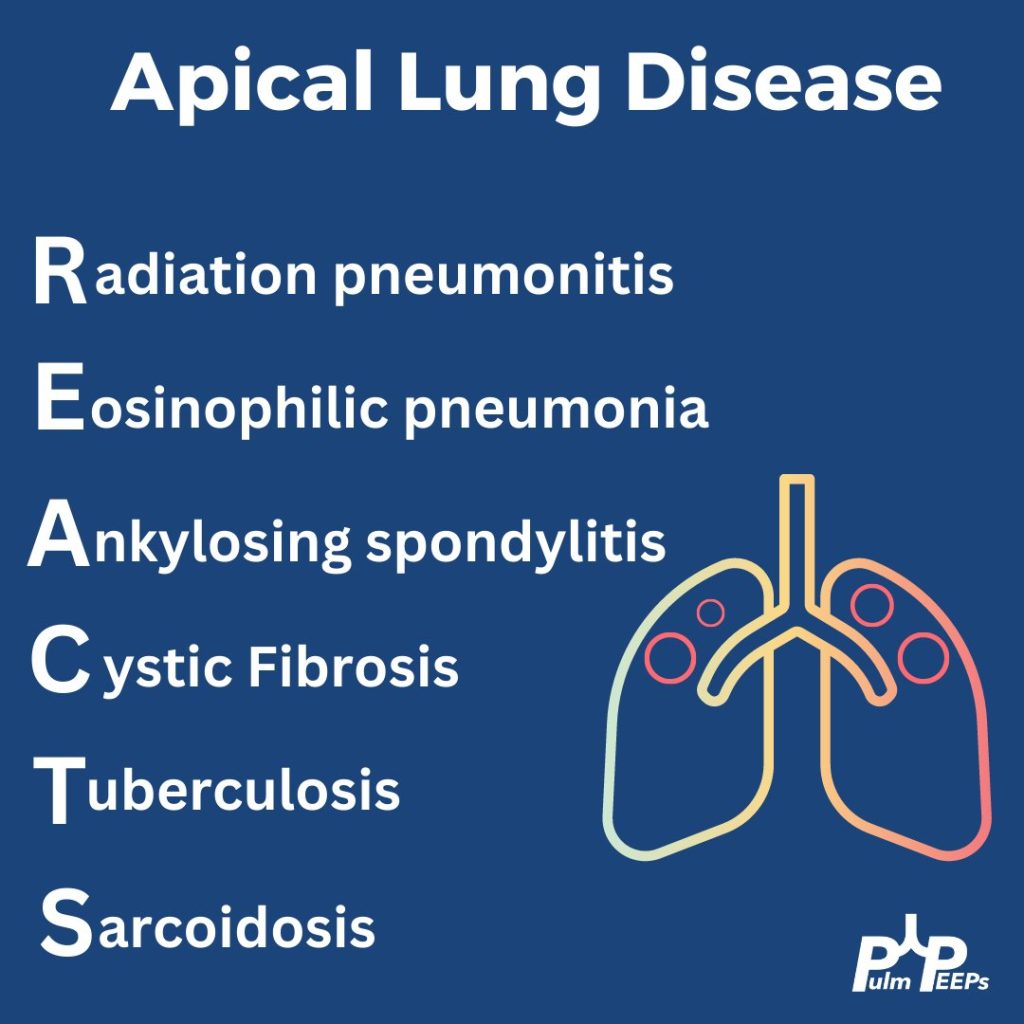
When thinking about apical lung disease, remember the mnemonic REACTS to help with your differential.
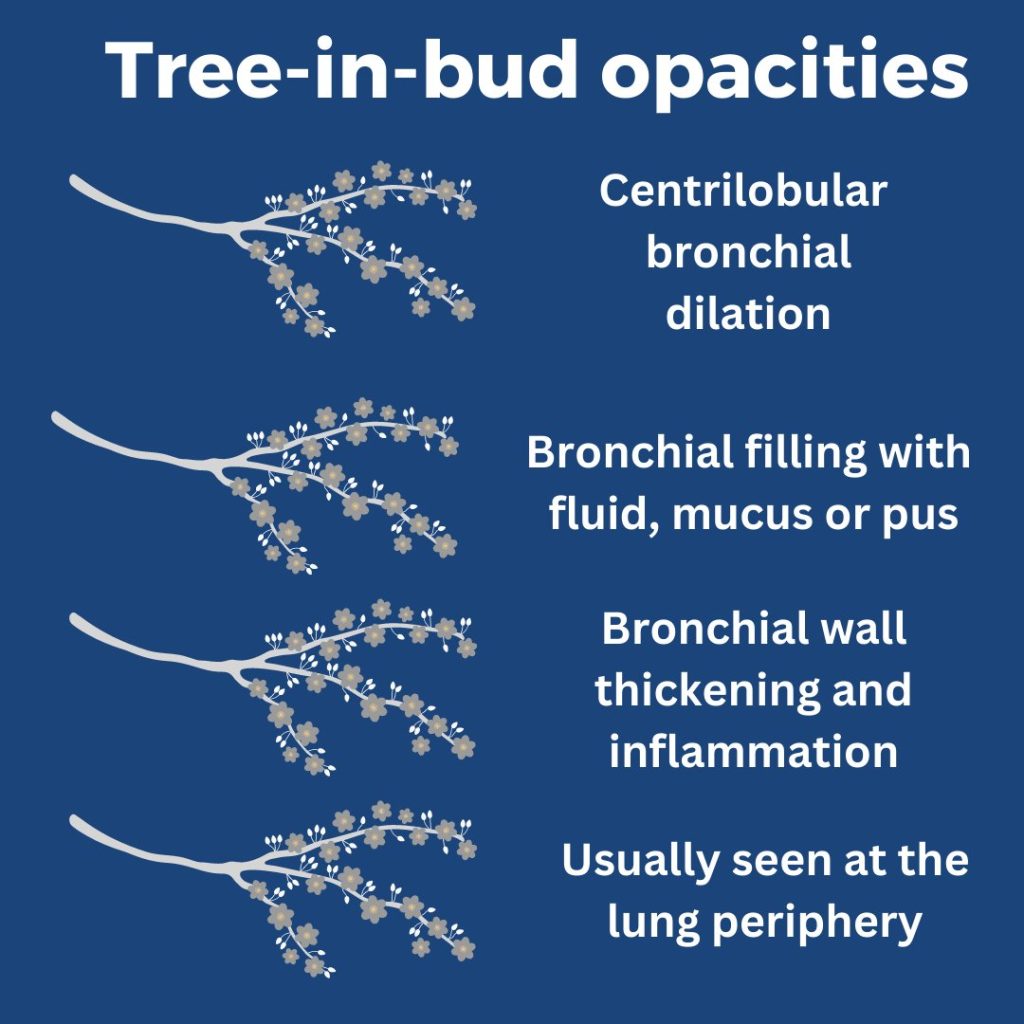
What are tree-in-bud opacities? They are findings seen on CT chest suggesting bronchial dilation, inflammation, and bronchial filling with fluid, mucus, or pus that can be caused by infections and non-infectious etiologies.
He had sputum and AFB cultures sent and his AFB smear was positive. He was ultimately diagnosed with disseminated TB and started on RIPE therapy.
Today we’re back with another stop on our Fellows’ Case Files journey. We’re at Boston University and Boston Medical Center with an outstanding fellow, the program director, and an expert guest to dive into a new case. Tune in to hear about this fascinating case and learn some key pulmonary points along the way.
Meet Our Guests
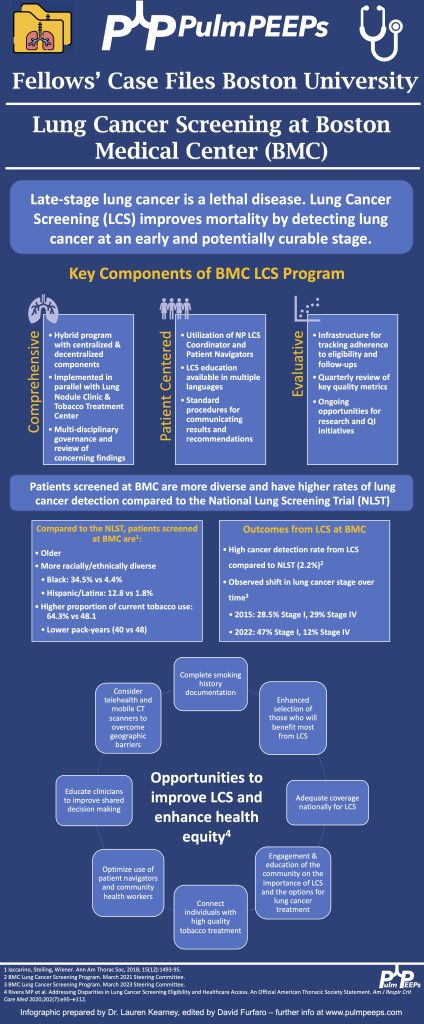
Lauren Kearney is a research fellow at Boston University. She completed her internal medicine residency and chief residency at BU. She is pursuing a research career in health equity and community-based participatory research to improve outcomes for patients with lung cancer and other pulmonary conditions.
Chris Reardon is a Clinical Professor of Medicine at Boston University, where she is also the Fellowship Training Program Director for Pulmonary and Critical Care Medicine. She is additionally the Director of Respiratory Care Services at Pappas Rehab Hospital for Children.
Katie Steiling is an Assistant Professor of Medicine at Boston University and a Member of the Bioinformatics Graduate Program. She founded the Lung Nodule Clinic at Boston Medical Center and co-chairs the Lung Cancer Screening Steering Committee. She is dedicated to improving the equitable treatment of patients with and at risk for lung cancer.
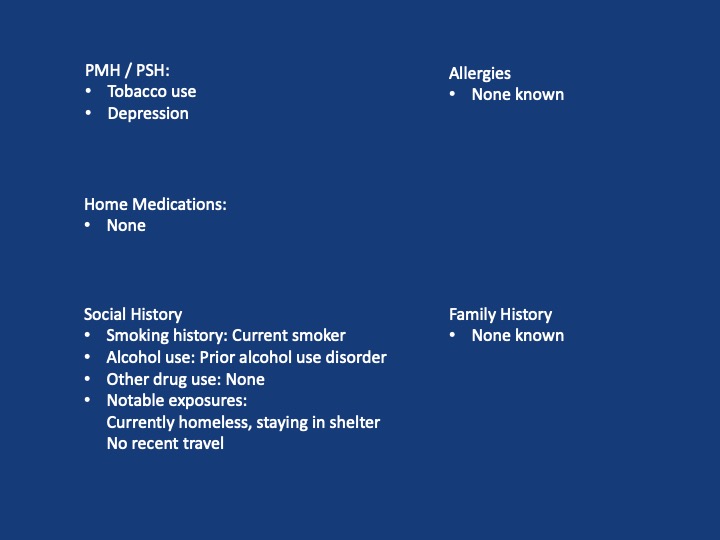
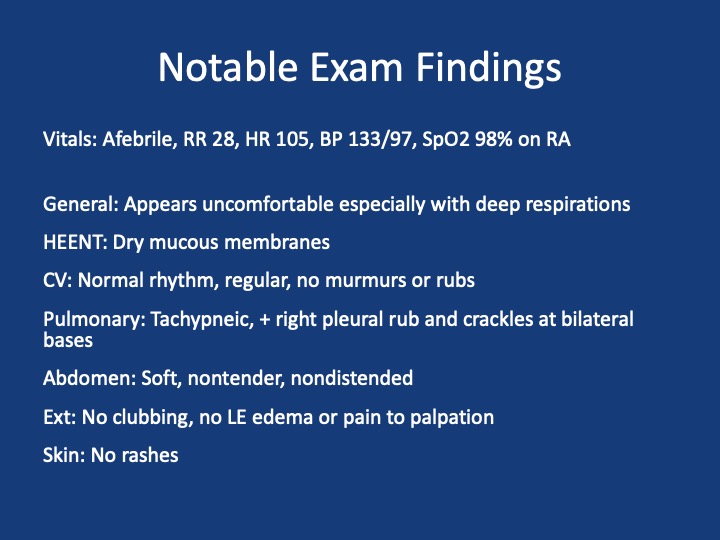
Case Presentation
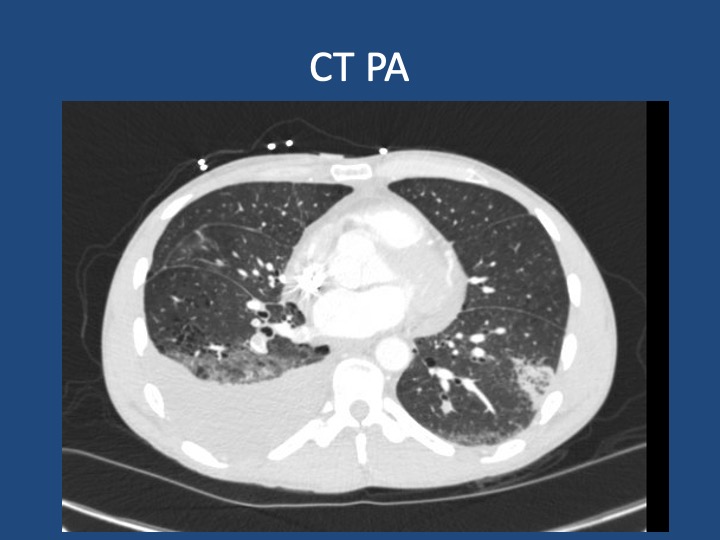
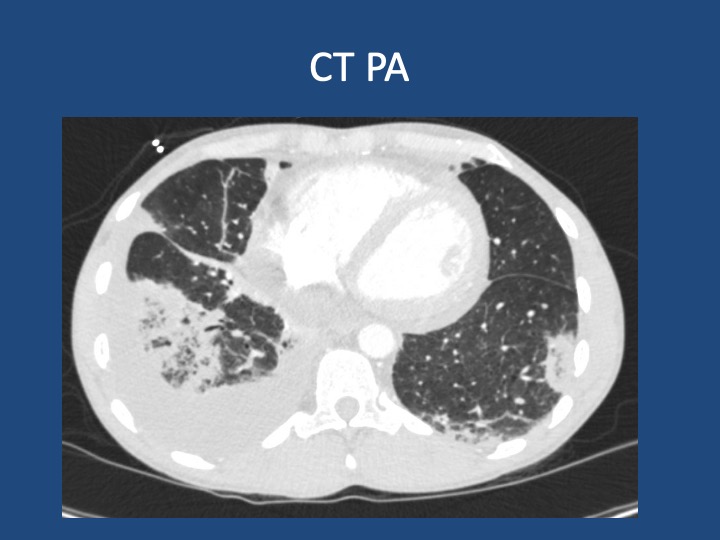
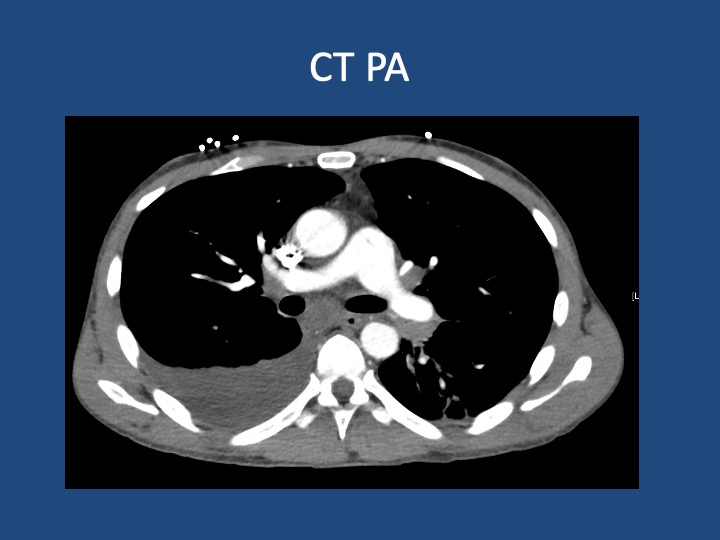
A 44-year-old man who is undomiciled and a current smoker presents with three days of intermittent, progressively worsening pleuritic chest pain with a cough productive of blood-tinged sputum. This is in the setting of 1-2 months of fatigue and anorexia, and 2 weeks of bilateral calf swelling.
Key Learning Points
Factors that may lead to initial hypercoagulability testing in first unprovoked PE: young age, thrombosis in multiple or unusual vascular beds, history of warfarin-induced skin necrosis, arterial thrombosis.
When lung cancer is suspected, identification of metastases to identify the highest radiologic stage and optimal biopsy site is essential.
Given that pleural fluid sensitivity is only ~46%, negative cytology should not assuage further malignancy work-up in a high-risk patient.
Black individuals in the US are at higher risk of developing and dying of lung cancer- the reasons for which are complex & multifactorial. Yet, gaps remain in the targeted identification of these patients, adequate lung cancer screening, and connection to diagnosis & treatment.