Listen in today to another stop on our Fellows’ Case Files journey. We’re at Northwestern University for another great case presentation. Tune in, check out our associated infographic, and let us know what you think!

Meet Our Guests
Jamie Rowell is a first-year clinical fellow in the Northwestern PCCM program. She completed medical school at the Medical University of South Carolina and her internal medicine residency and Chief Residency at the University of Vermont Medical Center.
Cathy Gao is an Instructor of Medicine at Northwestern and completed her PCCM fellowship there last year. Her research focuses on using machine learning applied to ICU EHR data to characterize patient trajectories and identify potential interventions to improve outcomes.
Clara Schroedl is an Associate Professor of Medicine in Pulmonary and Critical Care and Medical Education. She is the program director of the Northwestern PCCM fellowship program, with an interest in medical education and simulation.
Case Presentation
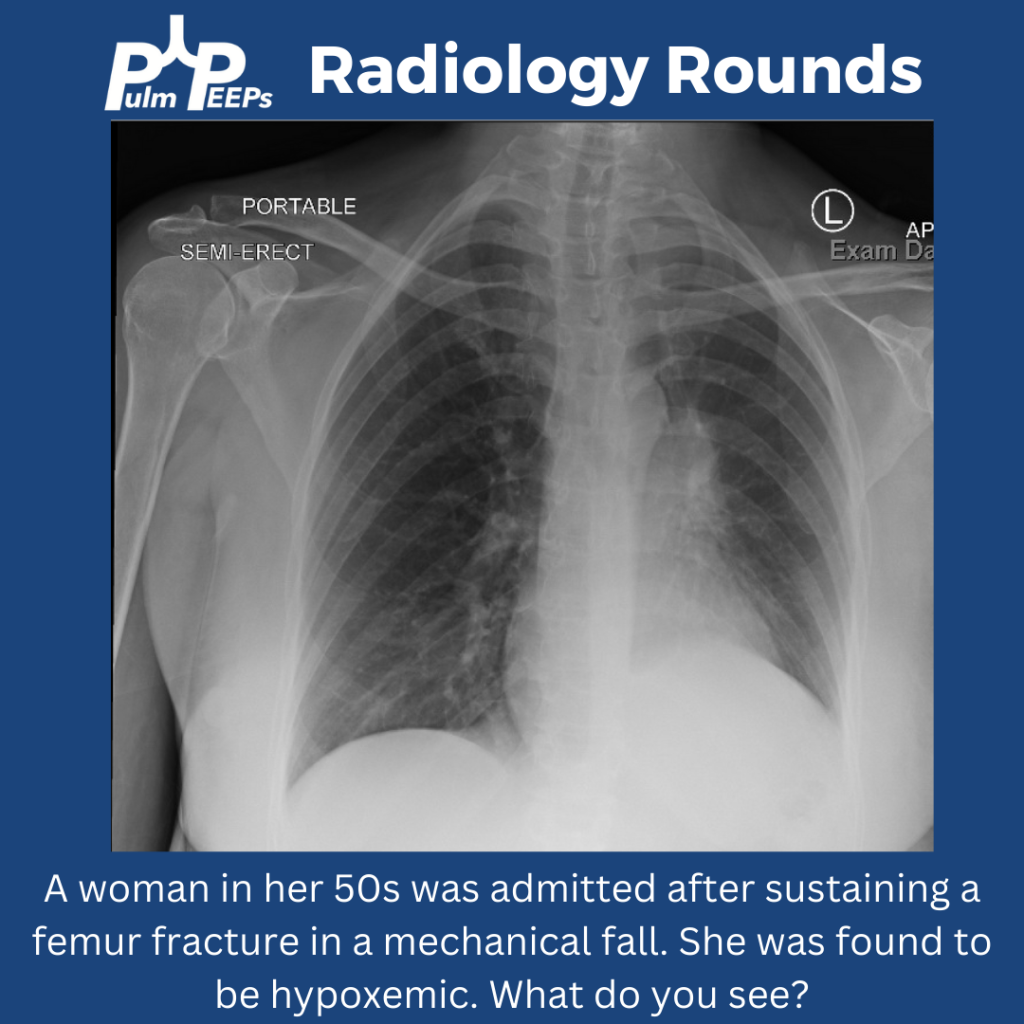
A 25-year-old previously healthy woman presents with recurrent episodes of right chest pain and cough. In October she was treated with antibiotics and felt somewhat better but in December, she presented again with chest pain, and again was treated with antibiotics. The pain improved but she still felt breathless. In February, again she had intense chest pain interfering with life, and was given NSAIDs and took high dose TID without clear benefit.
One month later, she coughed up some bloody mucus, so now she is presenting for evaluation. The chest pain is worse with deep breaths and improves in between these episodes. She only notes it on her right side. At this point, she does sometimes feel short of breath; she used to run 5 miles but is now struggling to run two miles. She denies any unusual exposures. She went to school in central rural Ohio for a while. She has no history of pulmonary infections, no exposure to mold or animals, and no history of vaping.
Key Learning Points
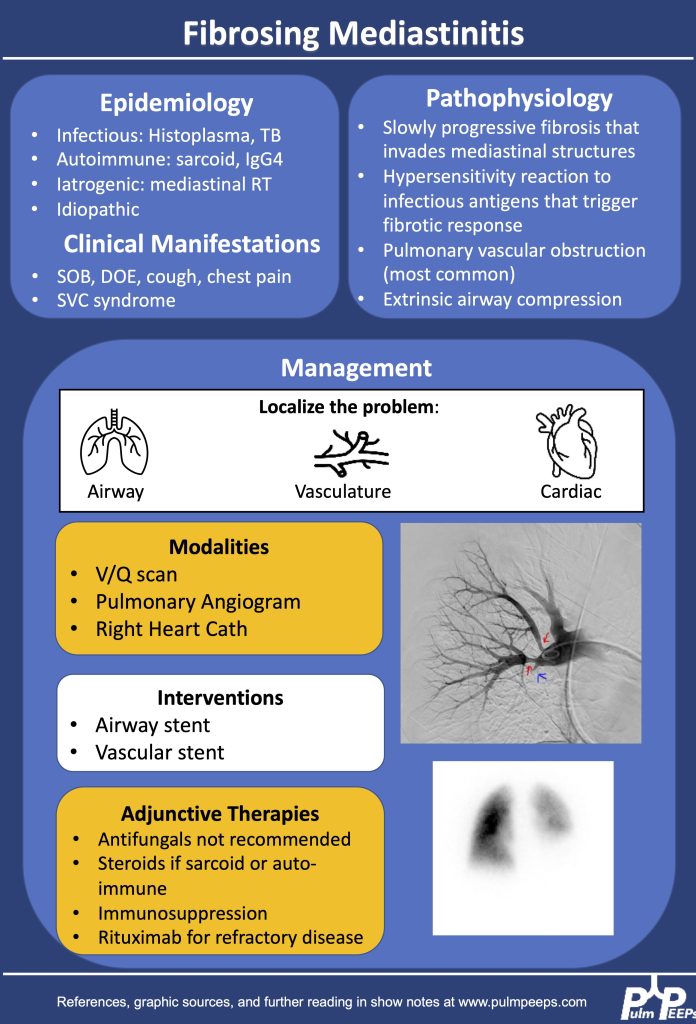
1.Making the diagnosis of Fibrosing Mediastinitis :
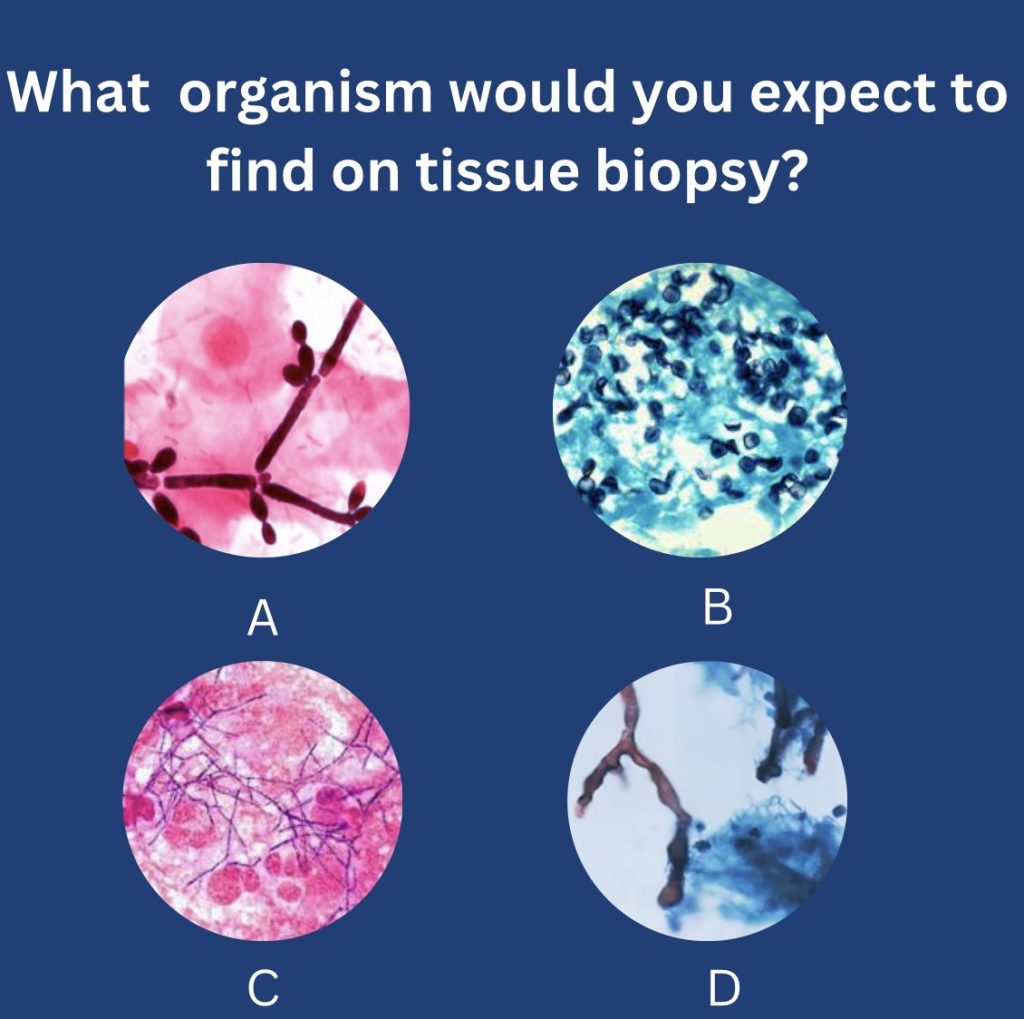
–Etiologies: histoplasmosis, sarcoidosis, tuberculosis, IgG4, Behcet, ANCA vasculitis
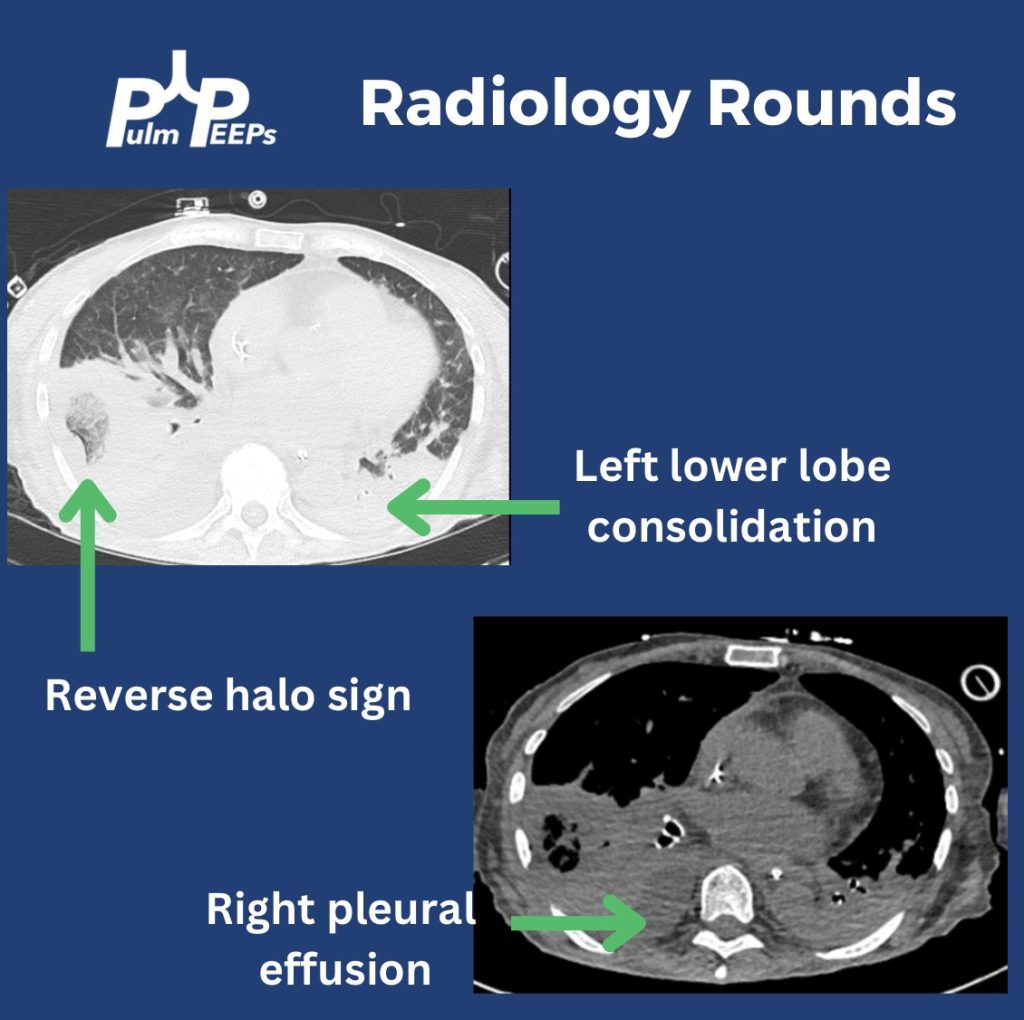
–Imaging modalities: CT chest, perfusion studies, pulmonary angiogram
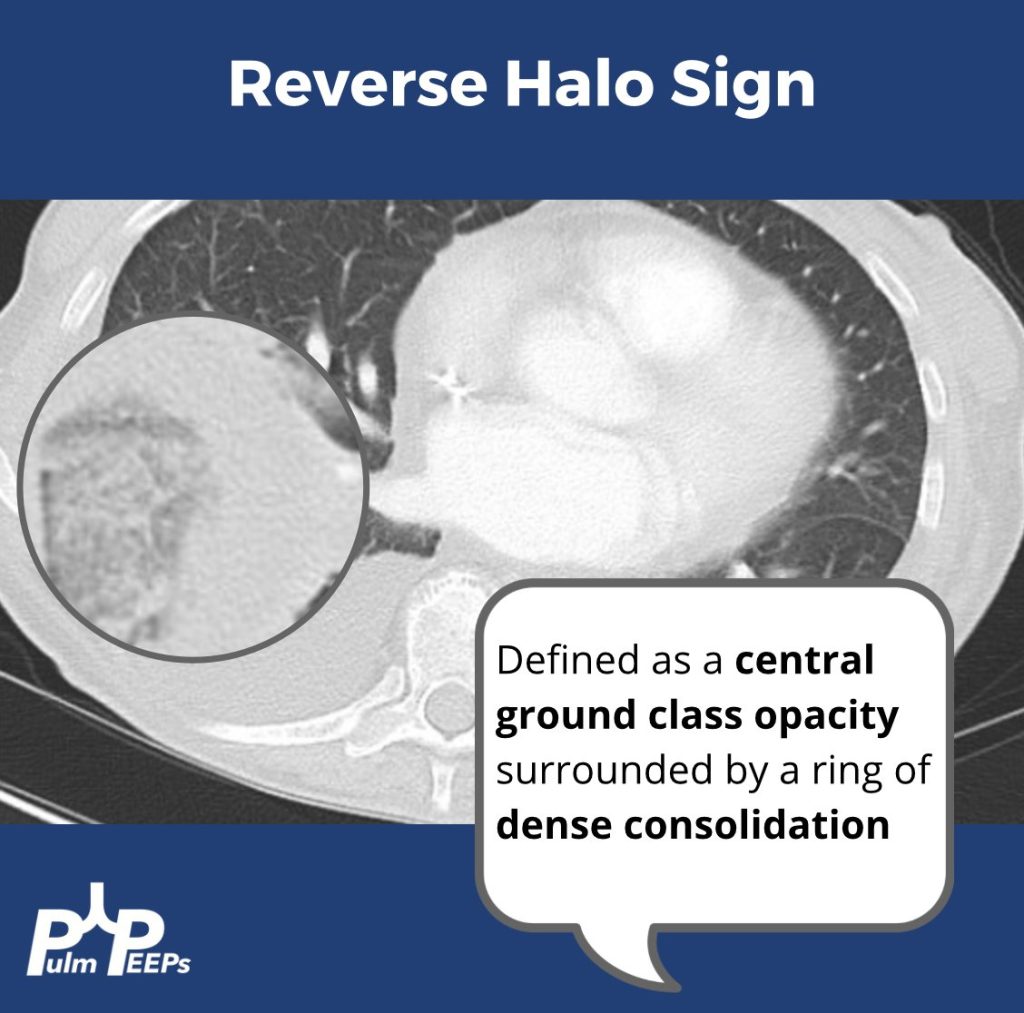
–Imaging characteristics: infiltrative, heterogeneous, fibrotic process that crosses fat planes and encroaches on nearby structures causing airway or vascular stenoses
2. Management strategies:
–No curative therapies. Goal to relieve symptom burden
–Airway stents
–Vascular stents
–Rituximab
–Antifungals, steroids generally not considered effective
References and Further Reading
Kern et al. Bronchoscopic Management of Airway Compression due to Fibrosing Mediastinitis. Annals of the American Thoracic Society 2017. 14: 1235-1359
Welby JP, Fender EA, Peikert T, Holmes DR Jr, Bjarnason H, Knavel-Koepsel EM. Evaluation of Outcomes Following Pulmonary Artery Stenting in Fibrosing Mediastinitis. Cardiovasc Intervent Radiol. 2021 Mar;44(3):384-391. doi: 10.1007/s00270-020-02714-z. Epub 2020 Nov 17. PMID: 33205295.
Westerly, BD Targeting B Lymphocytes in Progressive Fibrosing Mediastinitis. Am J Respir Crit Care Med. 2014 Nov 1; 190(9): 1069–1071.
https://rarediseases.org/rare-diseases/fibrosing-mediastinitis/#complete-report
https://pubmed.ncbi.nlm.nih.gov/21422386/
https://academic.oup.com/cid/article/30/4/688/421789
https://pubmed.ncbi.nlm.nih.gov/22033450/
https://www.sciencedirect.com/science/article/pii/S2352906715300087
https://www.atsjournals.org/doi/pdf/10.1513/AnnalsATS.201610-782RL
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS