We are excited to be back with a Rapid Fire Journal Club. Today’s episode is hosted by PulmPEEPs Associate Editor, Luke Hedrick, and will delve into the ANDROMEDA-SHOCK trial published in JAMA in 2019.
Meet our Guests
Jose Meade Aguilar is a second year Internal Medicine resident at Boston University Medical Campus (BUMC).
Article and Reference
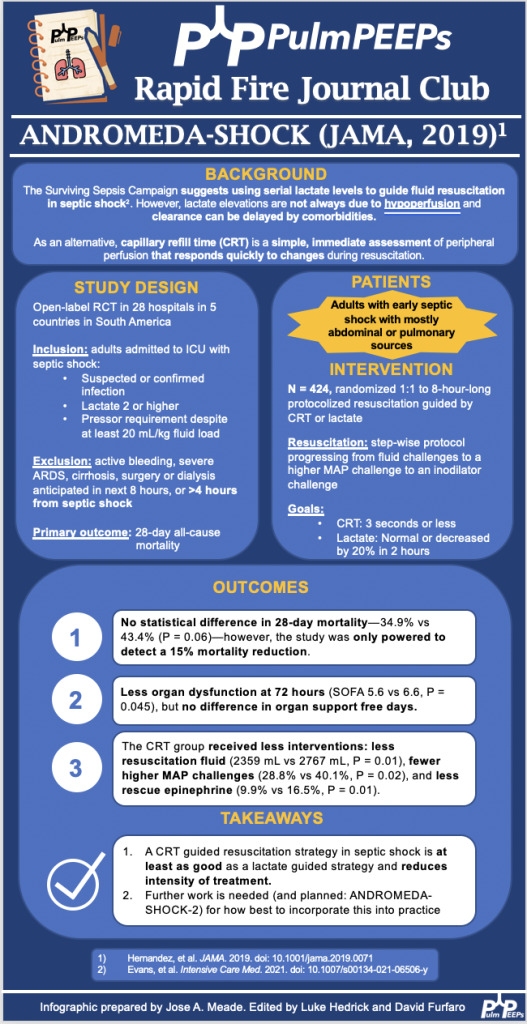
Today the discussion highlights the ANDROMEDA-SHOCK trial (JAMA, 2019) which evaluated whether resuscitation guided by capillary refill time (CRT) is superior to lactate-guided resuscitation in reducing mortality in patients with septic shock.
Our episode today is diving into a broader initiative to discuss the management of interstitial lung disease. In this episode we will be talking about the treatment of Idiopathic Pulmonary Fibrosis through the lens of a journal club discussion of the NEJM 2014 INPULSIS trial. Today’s episode is hosted by Pulm PEEPs Associate Editor Luke Hedrick.
Meet Our Guests
Robert Wharton is a recurring guest on Pulm PEEPs as a part of our Rapid Fire Journal Club Series. He completed his internal medicine residency at Mt. Sinai in New York City, and is currently a first year pulmonary and critical care fellow at Johns Hopkins.
Dr. Nicole Ng is an Assistant Profess of Medicine at Mount Sinai Hospital, and is the Associate Director of the Interstitial Lung Disease Program for the Mount Sinai National Jewish Health Respiratory Institute.
Article and Reference
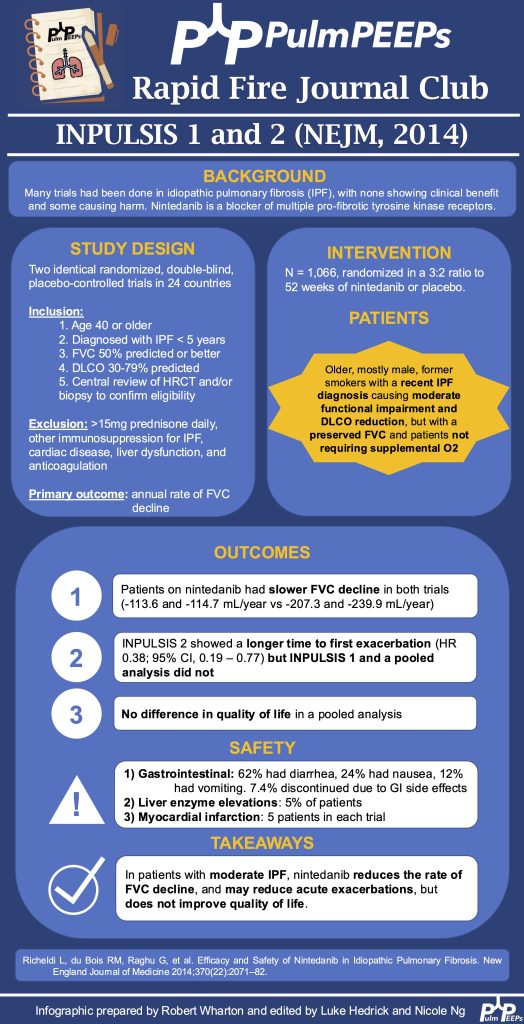
Today the discussion of IPF treatment centers around the 2014 NEJM publication of the INPULSIS trials investigating the efficacy of Nintedanib for the treatment of IPF.
Background and Challenges in ILD Treatment: Interstitial lung diseases (ILDs), particularly idiopathic pulmonary fibrosis (IPF), had historically poor treatment outcomes, with numerous therapies showing either no benefit or even harm. Prior to 2014, effective treatments were extremely limited, and lung transplantation was the primary management option.
INPULSIS I and II Trials: These 2014 trials examined nintedanib, an antifibrotic drug initially tested for cancer, in patients with moderate IPF. The studies were well-structured, involving strict criteria to ensure accurate diagnoses and excluding younger patients or those with more advanced disease.
Nintedanib’s Mechanism and Design of the Trials: Nintedanib acts by blocking multiple tyrosine kinases that mediate fibrotic growth factors. Patients were monitored over a year, with primary endpoints focusing on forced vital capacity (FVC) decline—a common surrogate measure for disease progression in ILD trials due to its correlation with survival.
Outcomes: Both trials showed that nintedanib significantly reduced the rate of FVC decline compared to placebo, suggesting that it slowed disease progression. Secondary endpoints included reduced acute exacerbations (significant only in one trial) and minor improvements in quality of life, though these weren’t statistically or clinically significant.
Adverse Effects: Nintedanib’s side effects included gastrointestinal issues (diarrhea, nausea, vomiting) and, less commonly, liver enzyme elevations and cardiovascular events. While post-marketing data suggested some improvements in tolerability, clinicians still monitor for these side effects closely.
Application in Clinical Practice: The trials support nintedanib as an option for slowing IPF progression, though no cure or disease reversal is achieved. Clinicians weigh the choice between nintedanib and pirfenidone (another antifibrotic) based on each drug’s side effect profile and individual patient needs.
Future Directions: The trials paved the way for further research into multi-therapy approaches for ILD, targeting multiple disease pathways, similar to strategies in asthma or COPD. Upcoming therapies and trials aim to provide more targeted and effective options for IPF and other ILDs.
We are joined today by two amazing educators from NYU for our latest Fellows’ Case Files Episode. Listen today as we go through a great case with some fantastic teaching points highlighted throughout the episode.
Meet Our Guests
Dr. Jeremy Grossman completed his Medicine-Pediatrics residency at Stony Brook Medicine where he was also a Chief Resident. He is currently a second-year PCCM fellow at NYU.
Dr. Shari Brosnahan is an Assistant Professor of Medicine and one of the Assistant Program Directors for the NYU Langone’s Division of Pulmonary, Critical Care, and Sleep Medicine. Her clinical and research interests are focused on pulmonary embolism and thrombosis in critically ill patients.
Case Presentation
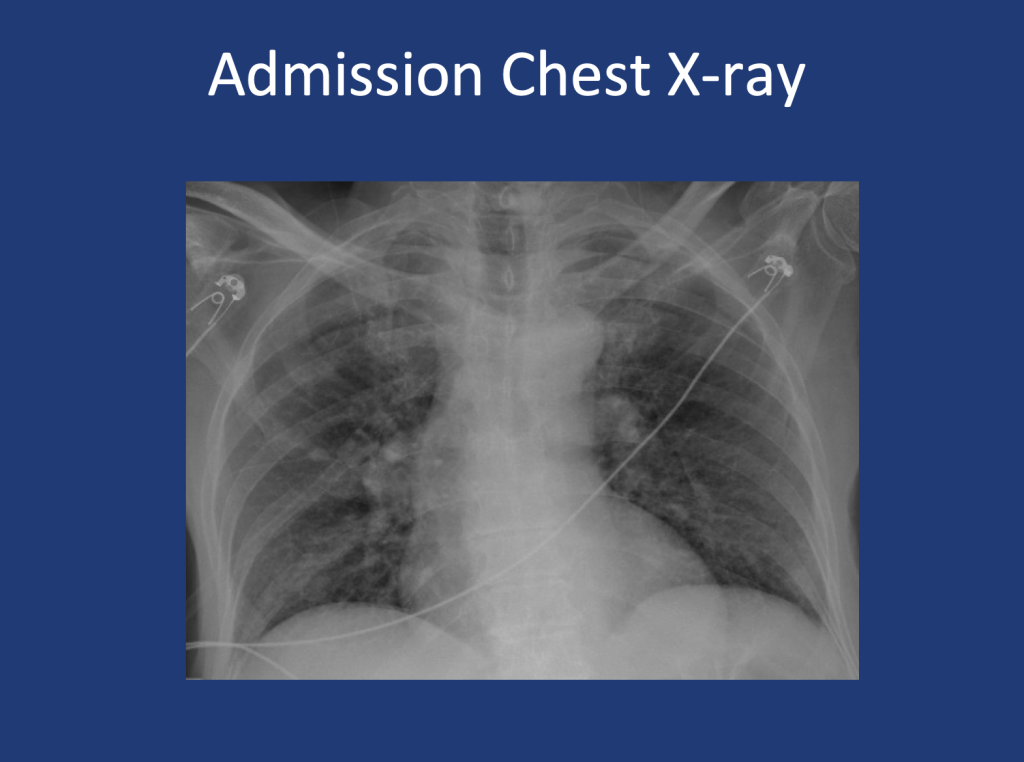
An 80-year-old male presents with shortness of breath. At home, his oxygen saturation was 82% on room air, improving only to 86% on 4L nasal cannula. Over the past month, he has experienced worsening symptoms, including a dry cough, fatigue, and difficulty speaking or ambulating due to shortness of breath at rest. He denies recent fever, sputum production, chest pain, or lower extremity swelling and presents to the ED for further evaluation.
Key Learning Points
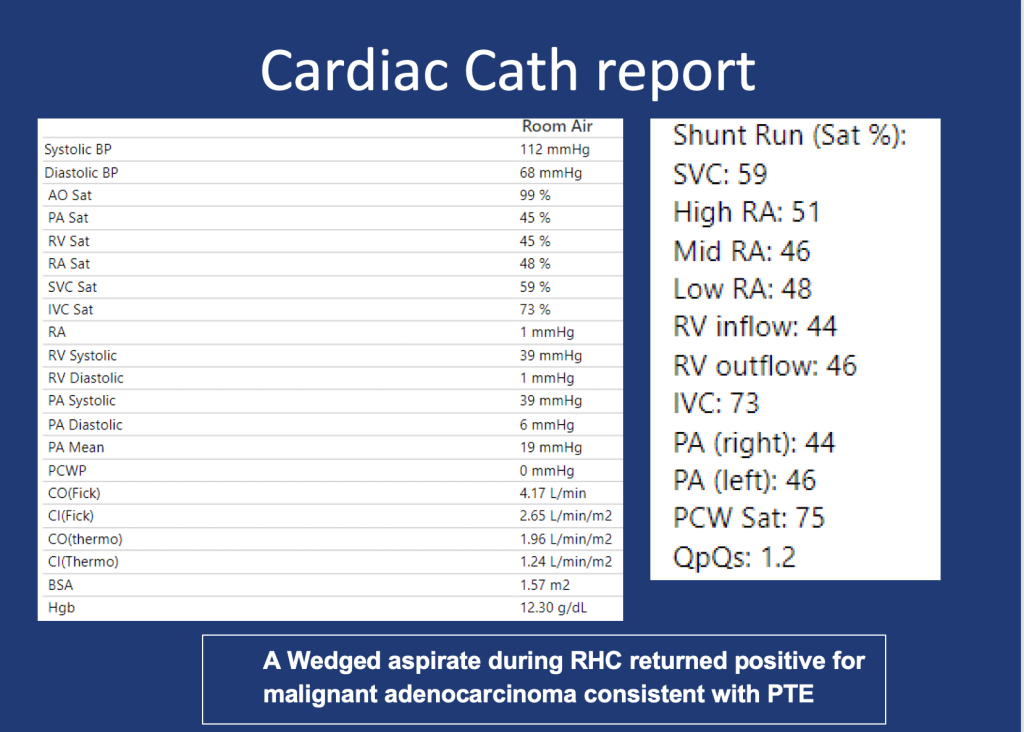
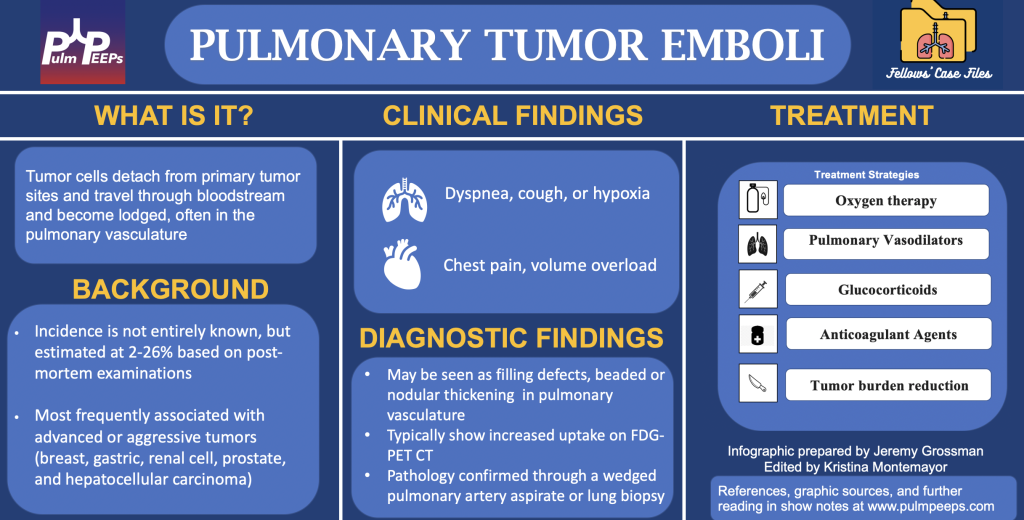
1.In any patient with a history of malignancy and hypoxia, clinicians should keep pulmonary tumor emboli (PTE) on the differential as early intervention may alter outcomes.
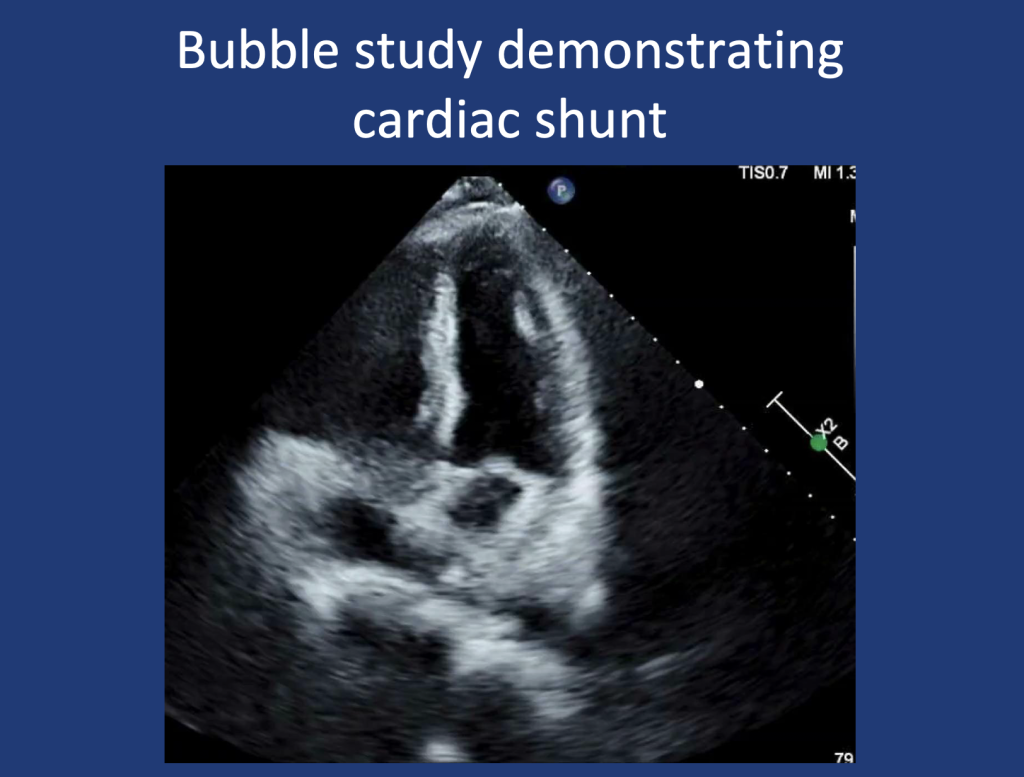
2.PTE contributes to hypoxia via mechanisms of mechanical obstruction of pulmonary arteries leading to shunting, VQ Mismatch, and in some cases pulmonary hypertension due to increased PVR.
3.A wedged aspirate can be used to diagnose PTE ante-mortem
Here at Pulm PEEPs we have always loved the CHEST Annual Meetings. We have enjoyed learning at them, reuniting with and meeting colleagues, and having conference specific episodes the past two years. This year, we had the opportunity to podcast live at CHEST 2024 and it was a real thrill! We talked to Maria Smilios about her wonderful book The Black Angels: The Untold Story of the Nurses Who Helped Cure Tuberculosis. . The book covers a range of fascinating topics including how treatments for tuberculosis were developed, the successes and plights of Black nurses working in this endeavor, an exploration of health care in New York City, and a discussion of Racism and civil rights in American healthcare.
We were also thrilled that Virginia Allen, the last surviving Black Angel is at the conference and her and her colleagues (posthumously) are receiving an honorary FCCP.
Meet Our Guests
Maria Smiios is a native New Yorker but completed her master of arts in religion and literature right here in Boston. She completed her masters at Boston University, where she was a Luce scholar, and taught in the religion and writing program. Through her work, she found a love for history, medicine and women’s narratives. While working at Springer Publishing as a science book editor, she learned about the story of the Black Angels and was determined to tell their story. She spent years deeply engaged in the lives and stories of those who were closest to these remarkable women.
We are excited to be back with our colleagues from CHEST to be previewing the CHEST 2024 Annual Meeting. CHEST his year is in Boston, MA from October 5th to October 9th. Listen in to hear about some great new features at CHEST this year, some old favorites, and to learn how to optimize your conference experience. See you all in two weeks!
Meet Our Guests
Sandhya Khurana is a Professor of medicine at University of Rochester school of medicine and Director of the Mary Parkes Asthma Center. Her clinical and research interest is in asthma. She is the Vice-Program Chair for CHEST 2024 and will be the program Chair for CHEST 2025 next year in Chicago.
Gabe Bosslet is the Program Chair for CHEST this year. In addition he is a Professor of Clinical Medicine at Indiana University School of Medicine. He is also an Assistant Dean at IU, and the Director of Mentoring and Faculty Development for the Division Pulmonary, Critical Care, Allergy and Occupational Medicine.
Huzaifah Salat is a clinician educator who is currently working as a consultant pulmonologist and intensivist at Advocate Aurora Health in Wisconsin. He completed his Pulmonary and Critical Care Fellowship at the University of Oklahoma Health Sciences Center
We are extremely excited today to announce a new collaboration with BMJ Thorax. Our mission at Pulm PEEPs is to disseminate and promote pulmonary and critical care education, and we highly value the importance of peer reviewed journals in this endeavor. Each month in BMJ Thorax, a journal club is published looking at high yield and impactful publications in pulmonary medicine. We will be putting out quarterly episodes in association with Thorax to discuss a journal club publication and synthesize four valuable papers. We hope you enjoy!
Meet Our Guests
Chris Turnbull is an Associate Editor for Education at Thorax. He is an Honorary Researcher and Respiratory Medicine Consultant at Oxford University Hospitals. In addition to his role as Associate Editor for Education at BMJ Thorax, he is also a prominent researcher in sleep-related breathing disorders.
Imran Howell is an Asthma Fellow at the Nuffield Department of Medicine, University of Oxford
To submit a journal club article of your own to Thorax, you can contact Chris directly – christopher.turnbull@ouh.nhs.uk
To engage with Thorax, please use the social media channels (Twitter – @ThoraxBMJ; Facebook – Thorax.BMJ) and subscribe on your preferred platform, to get the latest episodes directly on your device each month.
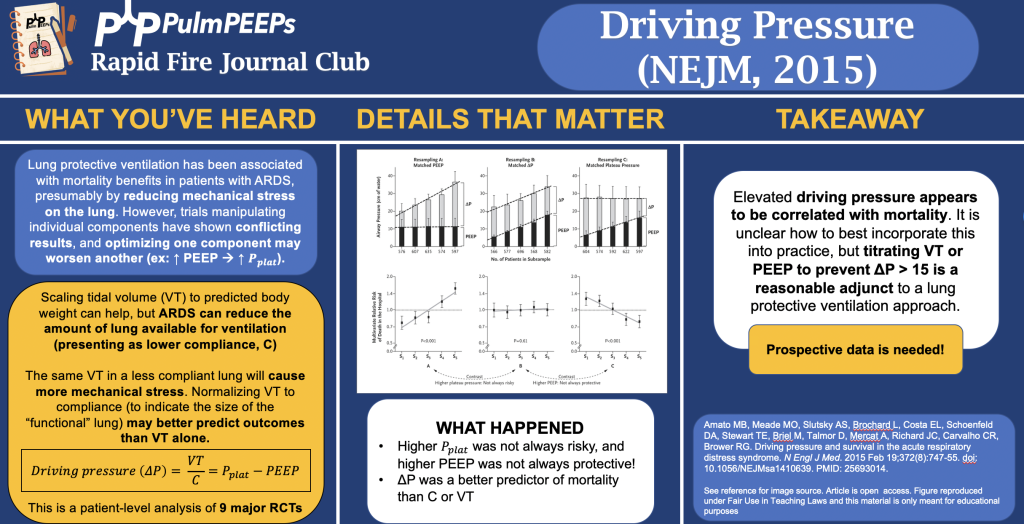
In this podcast episode, we continue our summer series reviewing landmark ARDS studies. Today, Dave and Luke discuss the Driving Pressure trial (published in NEJM in 2015) which evaluated the impact of driving pressure on survival in patients with ARDS.
Article and Reference
We are talking about the Driving Pressure trial today which evaluated the impact of driving pressure, as an independent variable, on survival in patients with ARDS.
In the penultimate episode in our ARDS Rapid Fire Journal Club Summer Series we are talking about the DEXA-ARDS trial (published in Lancet Respiratory Medicine in 2020). This trial evaluated the impact of dexamethasone in the treatment of ARDS.
Article and Reference
Today we’re discussing the DEXA-ARDS trial published in Lancet Respiratory Medicine in 2020. This trial evaluated the impact of dexamethasone on mortality and duration of mechanical ventilation for patients with ARDS.
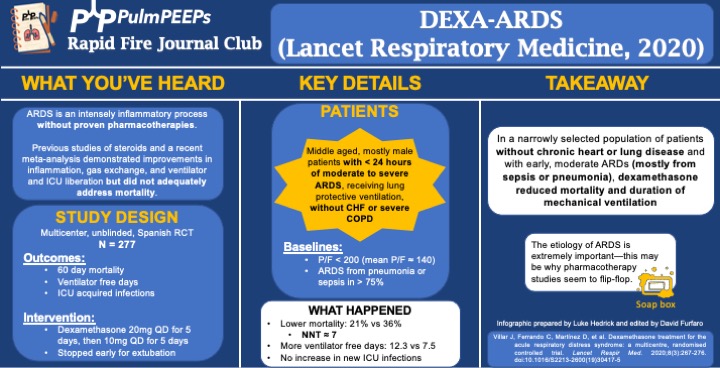
Background: ARDS is an intense inflammatory process without proven, specific pharmacotherapies. Previous work and a recent meta-analysis demonstrated improvements in inflammation, gas exchange, and ventilator and ICU liberation but did not adequately address mortality.
Study Design (design, primary outcome, participants, etc)
Design: investigator-initiated, multicenter, unblinded, randomized controlled trial in 17 academic ICUs in Spain, conducted from 3/2013 to 12/2018
Primary Outcome
VFD at 28d
Secondary:
60d mortality
Actual duration of ventilation in ICU survivors
ICU acquired infections
Participants
Inclusion ARDS with P/F < 200 for < 24hr on LTVV
Exclusion:
Already receiving steroids or immunosuppression
CHF
Severe COPD
DNR
Summary: Middle aged, mostly male patients with < 24hr of moderate to severe ARDS receiving LPV without chronic heart or lung disease
Like many ARDS trials, just over 3/4 of patients’ ARDS was caused by PNA or sepsis. Mean P/F was ~140
Intervention/Limitations
N = 277, stratified by center and then randomized
Intervention: dexamethasone 20mg qd for 5d followed by 10mg qd for 5d
Stopped early for extubation before day 10
First dose given no more than 30 hours after P/F < 200
Control: no placebo, just SOC
All patients received LTVV
Outcomes/Safety
Power: with N = 314 (actual N = 277), 80% power to detect 2 additional VFD and 15% mortality reduction
As an aside, this seems to be a theme in ICU trials: massively ambitious proposed benefits during power calculations and then under-enrolling for that power calculation ultimately resulting with a point estimate that favors the intervention but is not statistically significant.
Efficacy:
60d mortality: 21% vs 36%, P = 0.0047
NNT of just < 7!
VFD at 28d: 12.3 vs 7.5, P < 0.0001
Actual duration of ventilation in ICU survivors: 14.2d vs 19.5d (P = 0.0009)
Safety:
Hyperglycemia: 76% vs 70%, P = 0.33
Always interesting in steroid trials when no change in glucose control is seen. This isn’t the most EBM thing I’ll ever say, but frankly I disregard this and assume steroids will cause hyperglycemia regardless of the trial results.
ICU acquired infections: 24% vs 25%, P = 0.75
Takeaway
In a narrowly selected population of patients without chronic heart or severe lung disease and with early, moderate ARDS (mostly from sepsis or pneumonia), dexamethasone reduced mortality and duration of mechanical ventilation.
If time, insert soap-box about etiology of ARDS being very important (EG, flu, fungal, parasitic, mycobacterial infections)
We have another great case in our Fellows’ Case Files coming today from UMass Chan. Listen in for a great discussion about a fascinating case with interesting physical exam and radiographic findings.
Meet Our Guests
Dr. Jen Kodela completed her residency training at UMass Memorial Medical Center and is currently a third year PCCM fellow at UMass Chan.
Dr. Ariel McKenna completed her residency training at Maine Medical Center and is also currently a third year PCCM fellow at UMass Chan.
Dr. Will Wong is an Assistant Professor of Medicine and is the Program Director of the PCCM fellowship at UMass Chan
Case Presentation
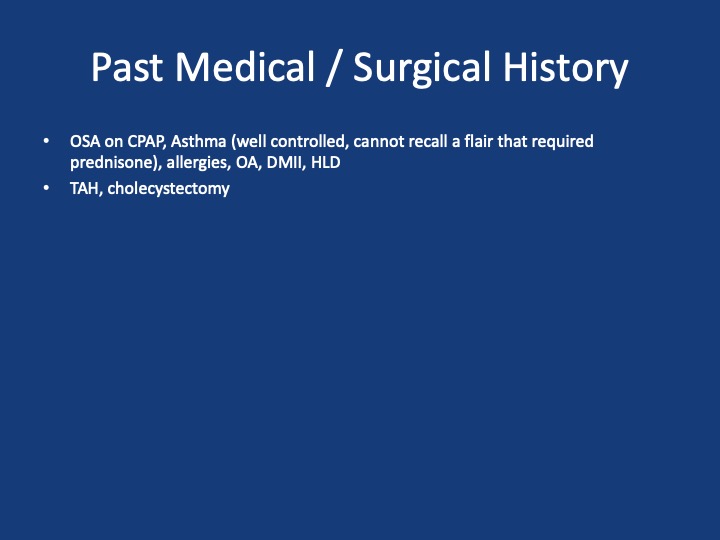
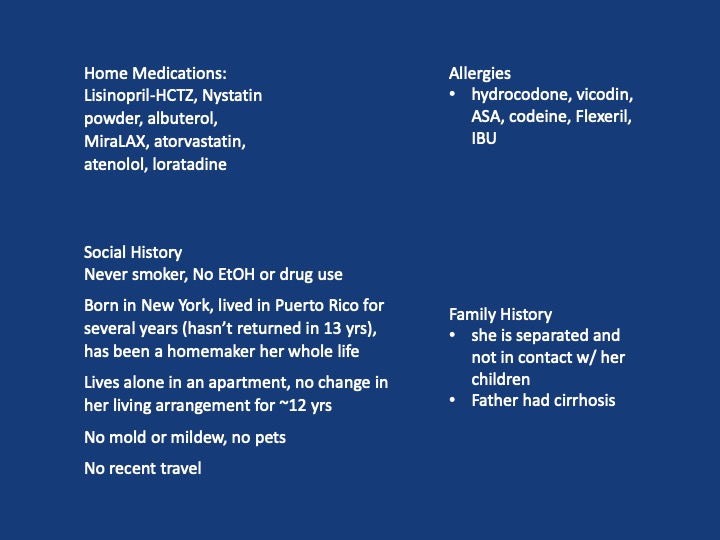
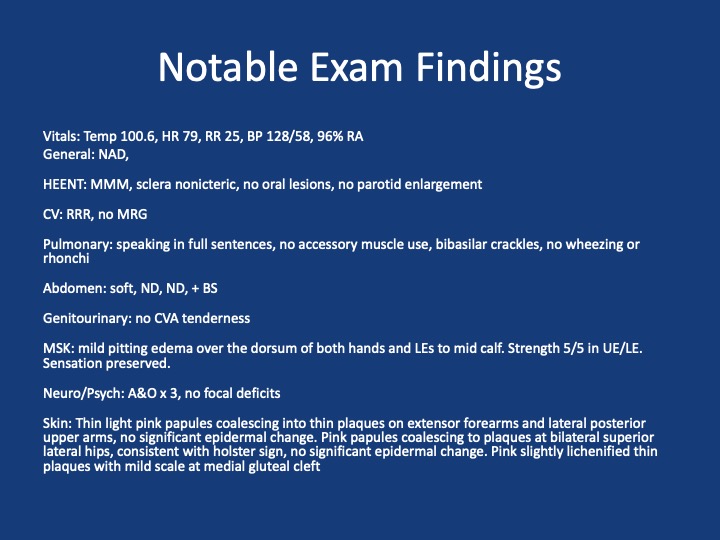
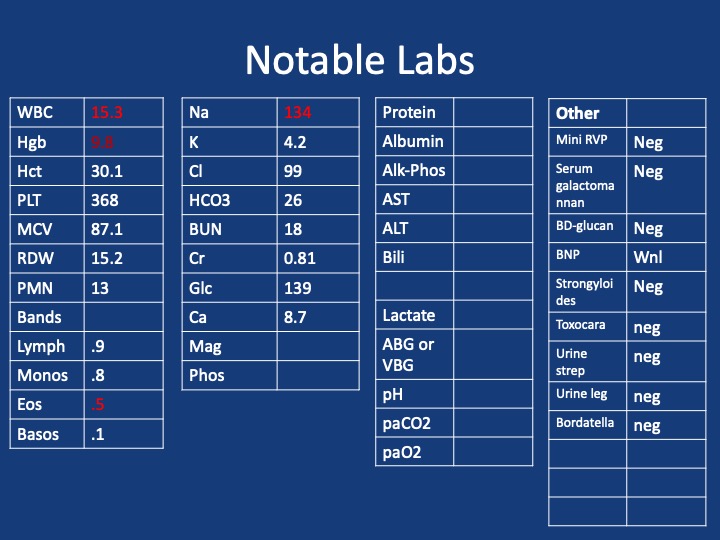
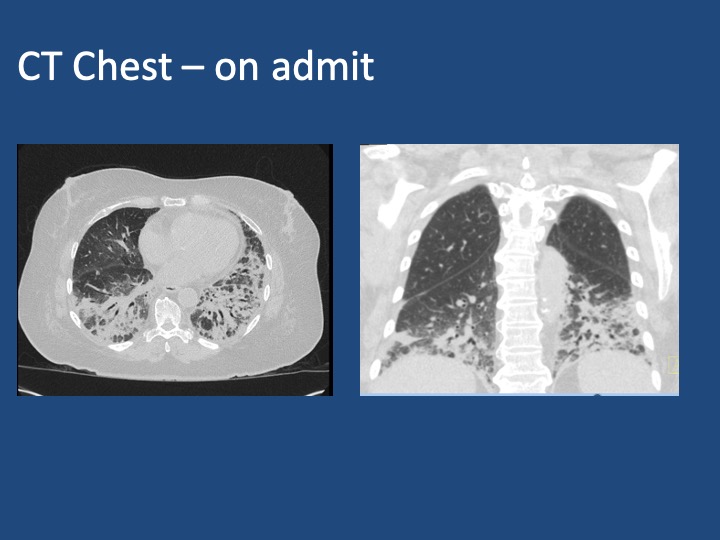
A 75 y/o F presenting with acute on chronic SOB, cough, L sided chest pain and rash. She has had ~7 months of progressive dyspnea, now a/w 2 months of productive cough, and several weeks of L sided chest pain and rash. She has been seen multiple times in the past two months for these sxs. During that time she received multiple antibiotic courses (urgent care, outpatient providers), including augmentin, azithromycin and levaquin, and asthma directed therapy (no steroids). Imaging throughout that time (CXRs, CTPE) show progression from a LLL infiltrate to bibasilar infiltrates. Despite these interventions, sxs continue to worsen. One month prior she was admitted to an OSH w/ continued worsening, vitals stable, exam nonfocal, mild leukocytosis but infectious w/u bland. Received broad spectrum abx. Bronch w/ BAL offers negative cultures, cytology, cell count w/ 66% neutrophils, 14% eosinophils. Discharged w/ dx of PNA on a 10 day course of levaquin and new exertional oxygen requirement of 2L. She then presents to Umass ~1 month later w/ continued progression of sxs
Key Learning Points
1. Formulate a differential diagnosis for non-resolving pneumonia
2. Evaluate the utility of transbronchial biopsy in the workup of undifferentiated ILD
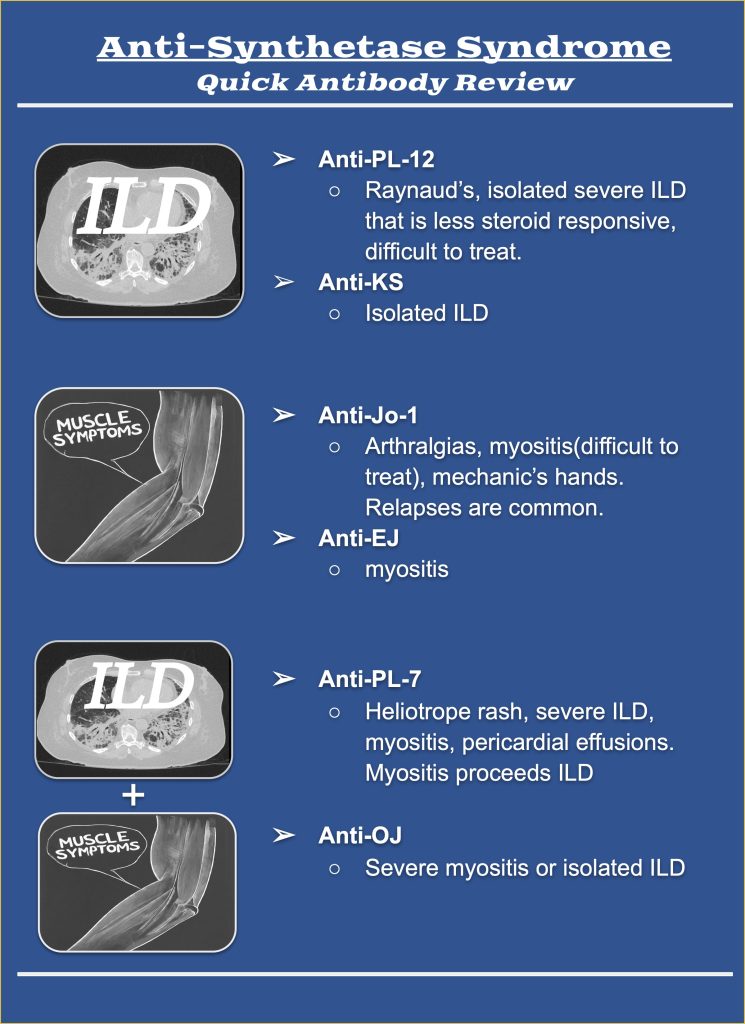
3. Describe the clinical manifestations of antisynthetase syndrome and identify the differences in presentation associated with PL-12 positivity
References and Further Reading
1. Kuru T, Lynch JP 3rd. Nonresolving or slowly resolving pneumonia. Clin Chest Med. 1999 Sep;20(3):623-51. doi: 10.1016/s0272-5231(05)70241-0. PMID: 10516909.
2. Troy LK, Grainge C, Corte TJ, Williamson JP, Vallely MP, Cooper WA, Mahar A, Myers JL, Lai S, Mulyadi E, Torzillo PJ, Phillips MJ, Jo HE, Webster SE, Lin QT, Rhodes JE, Salamonsen M, Wrobel JP, Harris B, Don G, Wu PJC, Ng BJ, Oldmeadow C, Raghu G, Lau EMT; Cryobiopsy versus Open Lung biopsy in the Diagnosis of Interstitial lung disease alliance (COLDICE) Investigators. Diagnostic accuracy of transbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): a prospective, comparative study. Lancet Respir Med. 2020 Feb;8(2):171-181. doi: 10.1016/S2213-2600(19)30342-X. Epub 2019 Sep 29. PMID: 31578168.
3. Hallowell RW, Danoff SK. Diagnosis and Management of Myositis-Associated Lung Disease. Chest. 2023 Jun;163(6):1476-1491. doi: 10.1016/j.chest.2023.01.031. Epub 2023 Feb 9. PMID: 36764512.
4. Hallowell RW, Paik JJ. Myositis-associated interstitial lung disease: a comprehensive approach to diagnosis and management. Clin Exp Rheumatol. 2022 Feb;40(2):373-383. doi: 10.55563/clinexprheumatol/brvl1v. Epub 2021 Mar 25. PMID: 33769263; PMCID: PMC8855729.
5. Marie I, Josse S, Decaux O, Dominique S, Diot E, Landron C, Roblot P, Jouneau S, Hatron PY, Tiev KP, Vittecoq O, Noel D, Mouthon L, Menard JF, Jouen F. Comparison of long-term outcome between anti-Jo1- and anti-PL7/PL12 positive patients with antisynthetase syndrome. Autoimmun Rev. 2012 Aug;11(10):739-45. doi: 10.1016/j.autrev.2012.01.006. Epub 2012 Feb 3. PMID: 22326685.
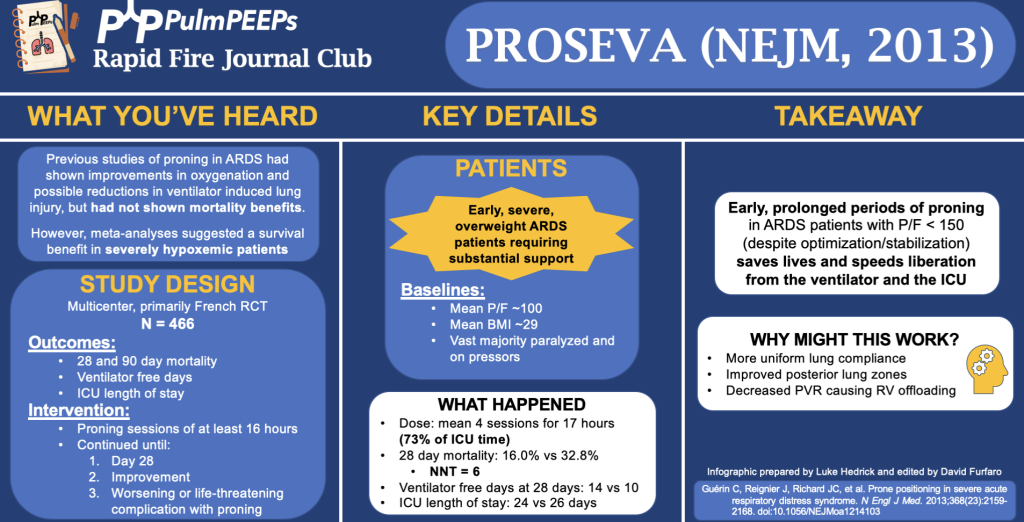
In this podcast episode, we continue our summer series reviewing landmark ARDS studies. Today, Dave and Luke discuss the PROSEVA trial (published in NEJM in 2013) which evaluated the impact of early, prolonged proning in patients with severe ARDS.
Article and Reference
We are talking about the PROSEVA trial today which evaluated the patients with severe ARDS (P/F < 150) to undergo prone-positioning sessions of at least 16 hours or to be left in the supine position.