We’re back with another Rapid Fire Journal Club. Luke Hedrick and Dave Furfaro discuss the NAVIGATOR trial published in NEJM in 2021 evaluating tezepelumab for adults with asthma.
Article and Reference
We are talking today about the NAVIGATOR trial evaluating the use of tezepelumab in adults with asthma.
Menzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, Brightling CE, Griffiths JM, Hellqvist Å, Bowen K, Kaur P, Almqvist G, Ponnarambil S, Colice G. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N Engl J Med. 2021 May 13;384(19):1800-1809. doi: 10.1056/NEJMoa2034975. PMID: 33979488.
https://www.nejm.org/doi/full/10.1056/NEJMoa2034975
Key Learning Points
Background & Rationale
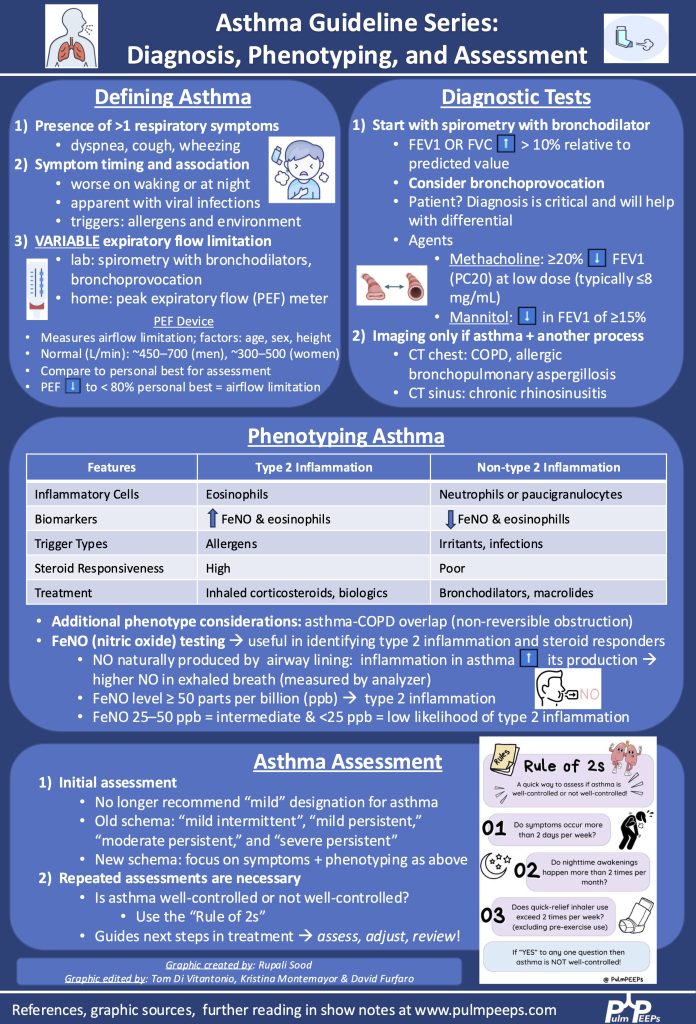
- Asthma biologics already exist, targeting IgE and type 2 cytokines (IL-4, IL-5, IL-13), but there’s an unmet need for patients with non-allergic or non-eosinophilic phenotypes.
- Tezepelumab is a monoclonal antibody targeting TSLP (thymic stromal lymphopoietin), an upstream mediator of both T2 and non-T2 inflammation, offering a potentially broader therapeutic effect.
📌 Study Design (Navigator Trial)
- Phase 3, double-blind, placebo-controlled RCT
- Conducted in 18 countries from 2017-2020
- N = 1,061 patients, aged 12-80 with moderate to severe asthma
- All were on medium/high-dose ICS + controller med
- Required ≥2 exacerbations in prior year
📌 Outcomes
- Primary Outcome: Annualized rate of asthma exacerbations (events per patient-year)
- Secondary Outcomes:
- Change in pre-bronchodilator FEV₁
- Symptoms & quality of life (with predefined MCIDs)
- Subgroup analyses by eosinophil count, FeNO, and perennial allergen sensitivity
📌 Key Inclusion/Exclusion
- Inclusion: 12-80 years, guideline-based therapy, ≥2 exacerbations
- Exclusion: recent biologic use, mild/asymptomatic asthma, no reversibility on spirometry
📌 Patient Population (Table 1 Summary)
- Middle-aged, predominantly white, female
- Poorly controlled severe asthma despite high-intensity therapy
- ~75% on high-dose ICS, ~10% on oral steroids
- ~40% had normal FeNO
- ~60% had eosinophils <300
- Median IgE ~195
Results
Efficacy:
- Annualized exacerbation rate:
- 0.93 (tezepelumab) vs. 2.1 (placebo)
- Rate ratio: 0.44, p<0.001 (very positive)
- In eosinophils <300 group: rate ratio 0.59, still effective
- FEV₁ improved by ~+0.25 L (vs. +0.09 L placebo), significant & sustained from week 2 onward
- Quality of life: statistically improved but did not meet MCID, so unclear clinical impact
- Severity of exacerbations reduced: fewer hospitalizations & ED visits in the treatment arm
- ~40% of treated patients still had some exacerbations → not a cure, but improves severity
Safety:
- Very well tolerated
- 77% reported adverse events (more common in placebo)
- No anaphylaxis, no GBS, no cancer signal
- Most common AEs: URTI, headache, nasopharyngitis
- Injection site reactions: 3.6%
- Serious AEs were lower in drug arm than placebo
Overall Takeaway
- Tezepelumab significantly reduces asthma exacerbations (including in patients with low eosinophils), improves lung function, and is safe and well tolerated.
- Provides a broad-acting biologic option even for patients who may not be eligible for existing T2-high biologics.
- Now widely used as part of the asthma biologic armamentarium for poorly controlled asthma despite maximal inhaled therapy.
Infographic:

Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Amazon Music | Android | iHeartRadio | Podcast Index | RSS