Today’s #RadiologyRounds is a reminder that pulmonary care extends beyond the lungs! Although we’ll have a CT chest too
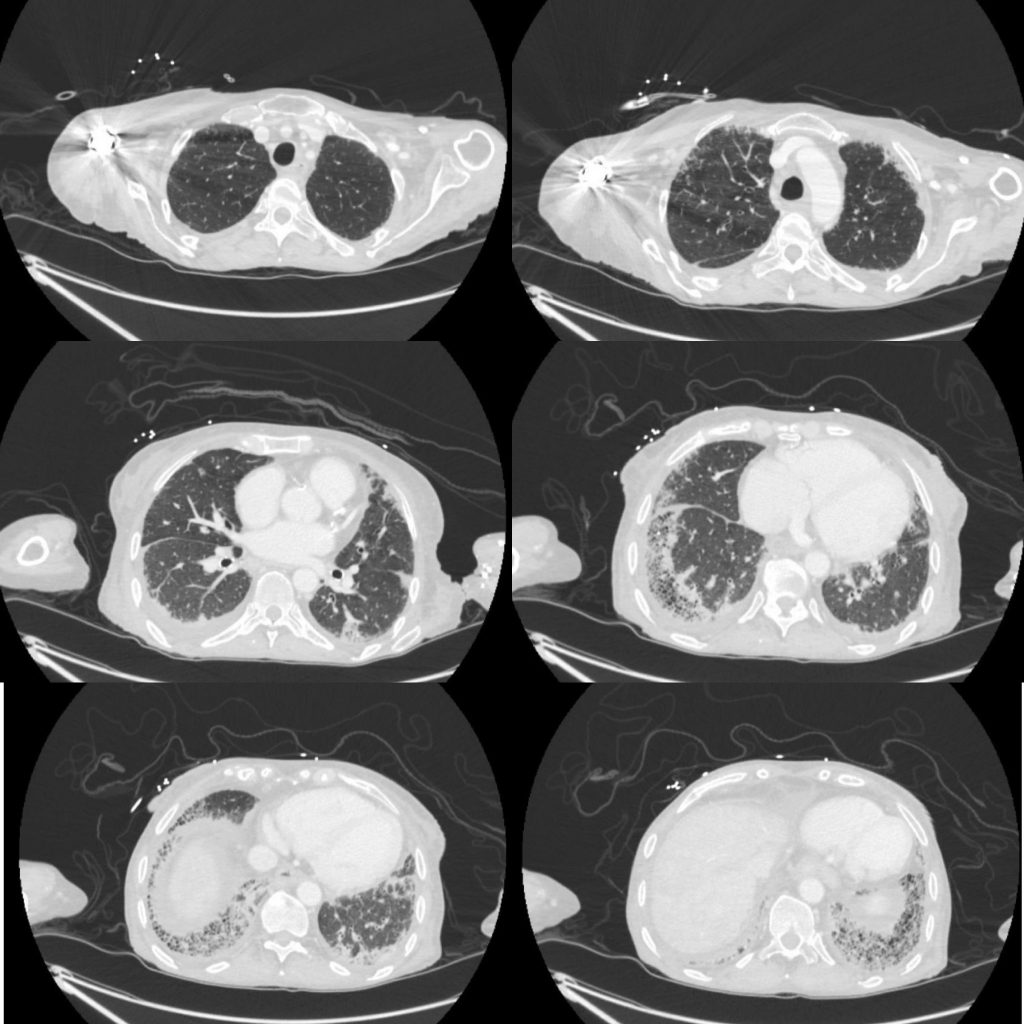
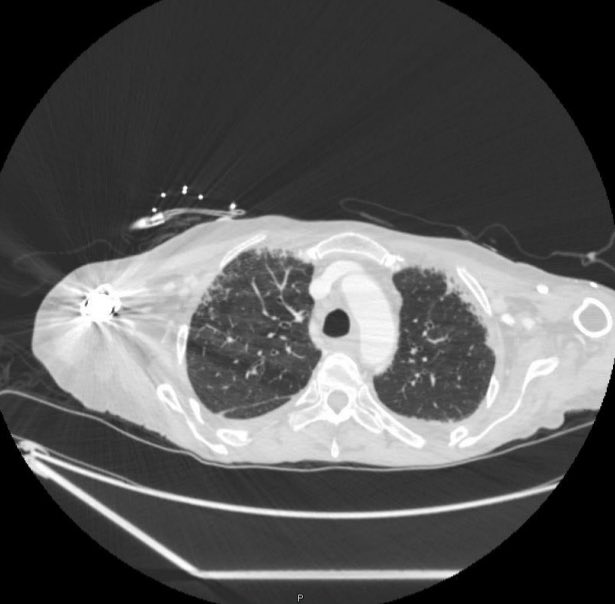
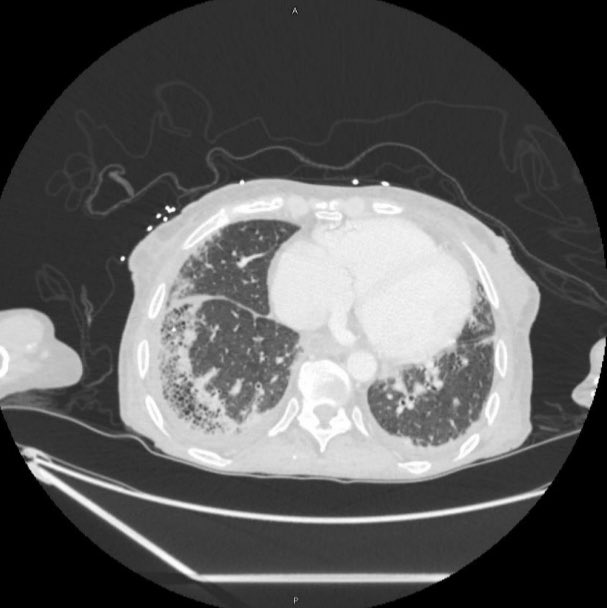
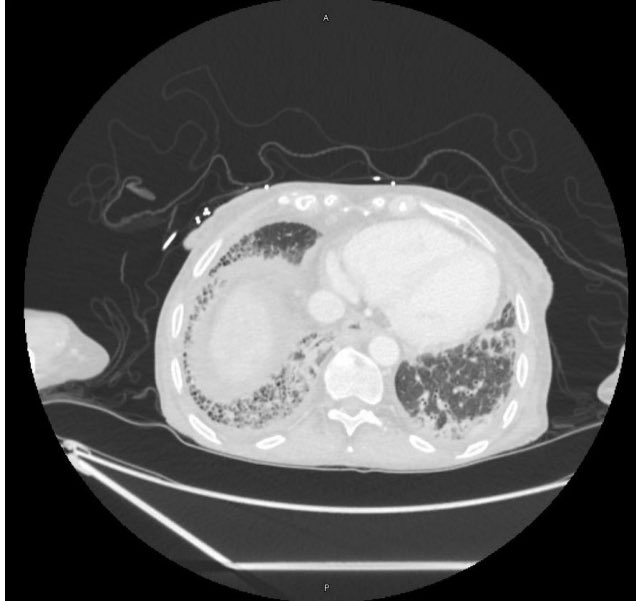
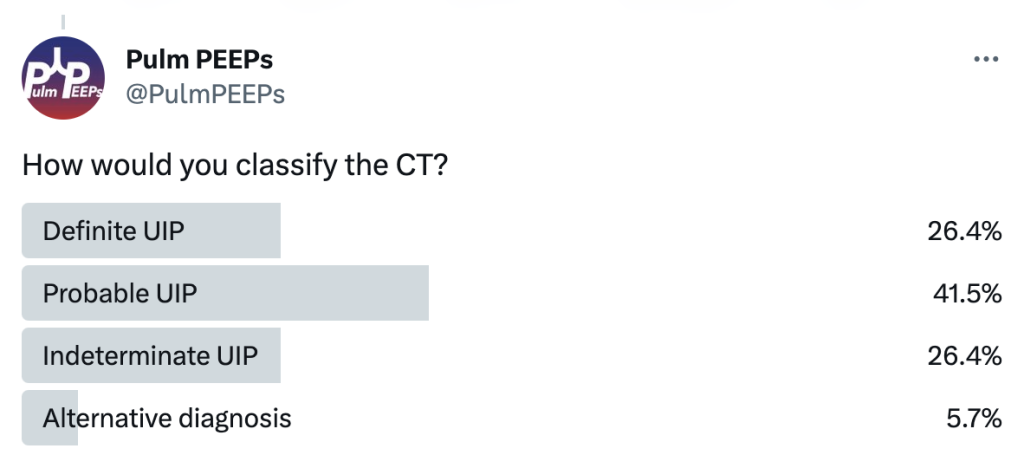
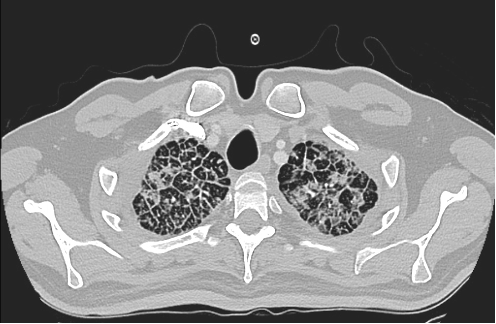
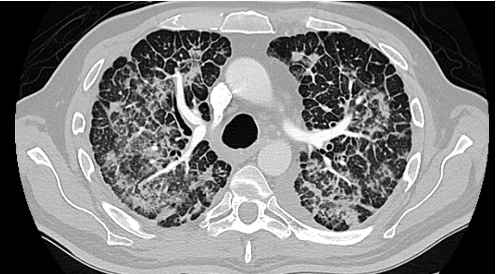
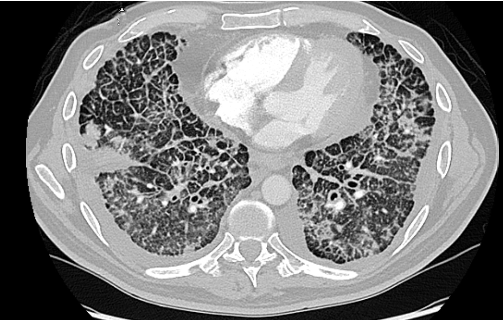
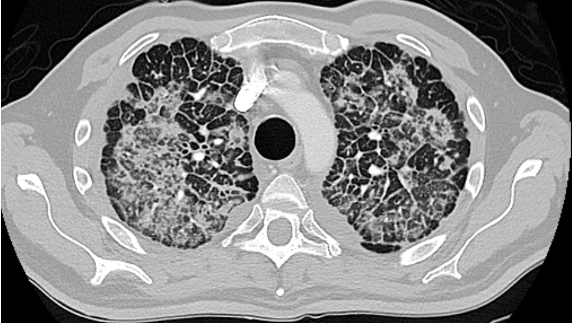
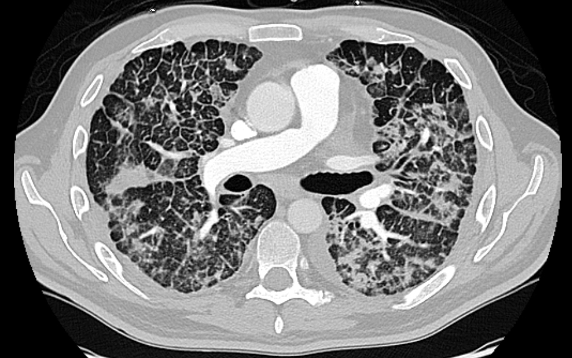
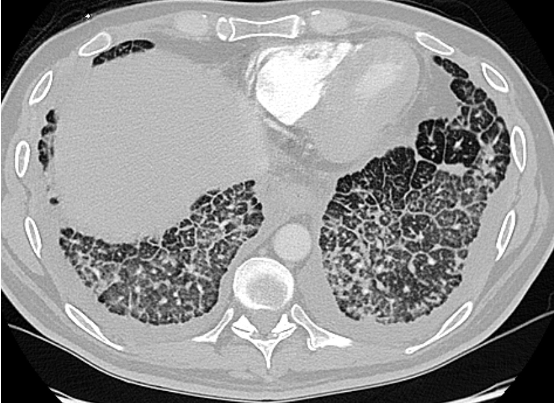
A 70-year-old woman with a diagnosis of seronegative RA presents with progressive dyspnea. PFTs show a moderate restrictive defect and moderately reduced DLCO. Here is the CT scan:
The CT was interpreted as indeterminate for UIP / fibrosing NSIP. The basilar and subpleural fibrosis and honeycombing are consistent with UIP, but with reticular nodular infiltrates and pleural effusions that are less consistent. In reviewing her history: RF, CCP, and anti-SCL70 were all negative. On hand exam, she had MCP enlargement, some PIP synovitis, and slight R hand ulnar deviation. She did not have clear telangiectasias. She had a history of GERD. She denied Raynauds. She had significant skin thickening over her legs and limited ankle mobility. X-rays were obtained:
This showed severe dystrophic calcifications and no bony erosions. This degree of extensive dystrophic calcifications is consistent with scleroderma and the patient was felt to have limited scleroderma, and possibly an overlap syndrome
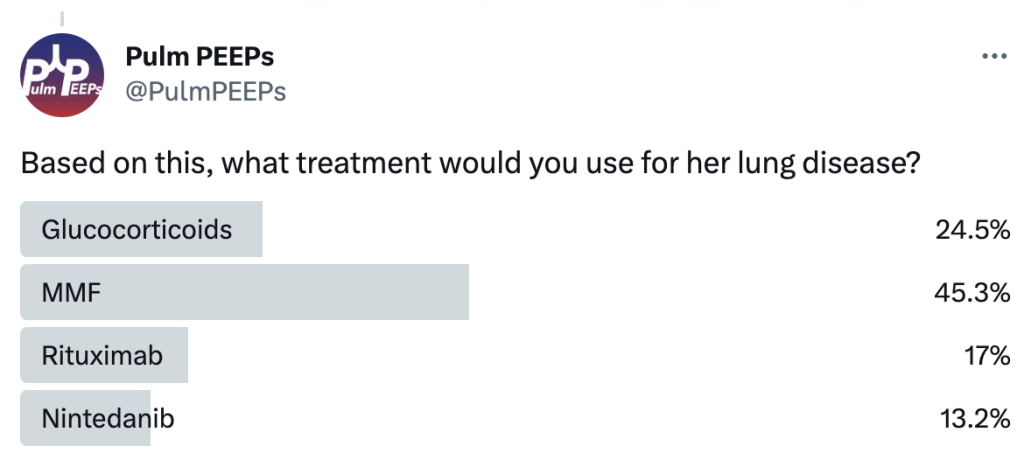
The patient was started on MMF as the initial agent based on the Scleroderma Lung Study II (SLSII): https://pubmed.ncbi.nlm.nih.gov/27469583/ Glucocorticoids were avoided given the risk of scleroderma renal crisis with steroids. An anti-fibrotic was also considered but not started as 1st line.
Join us as we head to Indiana University! Listen in as we discuss another great case and hear teaching points from our amazing guests.
Meet our Guests
Parth Savsani is currently an internal medicine resident at Indiana University School of Medicine. He received his undergraduate degree from the University of Wisconsin-Madison and his medical degree from the University of Illinois College of Medicine. He enjoys medical education and was selected to be the VA chief resident next year.
Maria Srour is a Pulmonary and Critical Care Fellow at Indiana University School of Medicine. She completed her internal medicine residency at Saint Louis University where she was also a chief resident, and received her medical degree from IU. She works in global health to improve care for sepsis patients in low resources settings, and is currently pursuing her MPH.
Laura Hinkle is a Indiana University die hard and has been there from her since medical school through residency and fellowship, and is now an Assistant Professor of Clinical Medicine and the Associate Program Director for the Pulmonary and Critical Care Medicine Fellowship. She will be taking over as the Program Director July 1, 2023. She is a dedicated educator and is the Key Clinical Educator for Pulmonary and Critical Care, and the Director of the Clinical Transitions Curriculum. Additionally, she is working on a Master’s Degree in Education through the University of Cincinnati.
Case Presentation
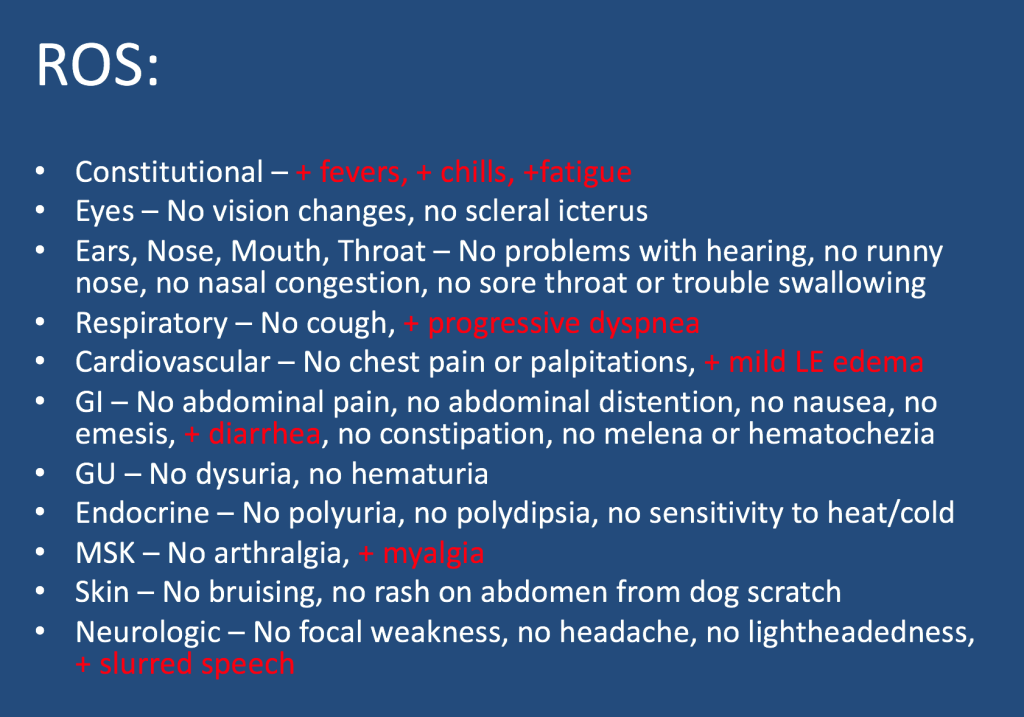
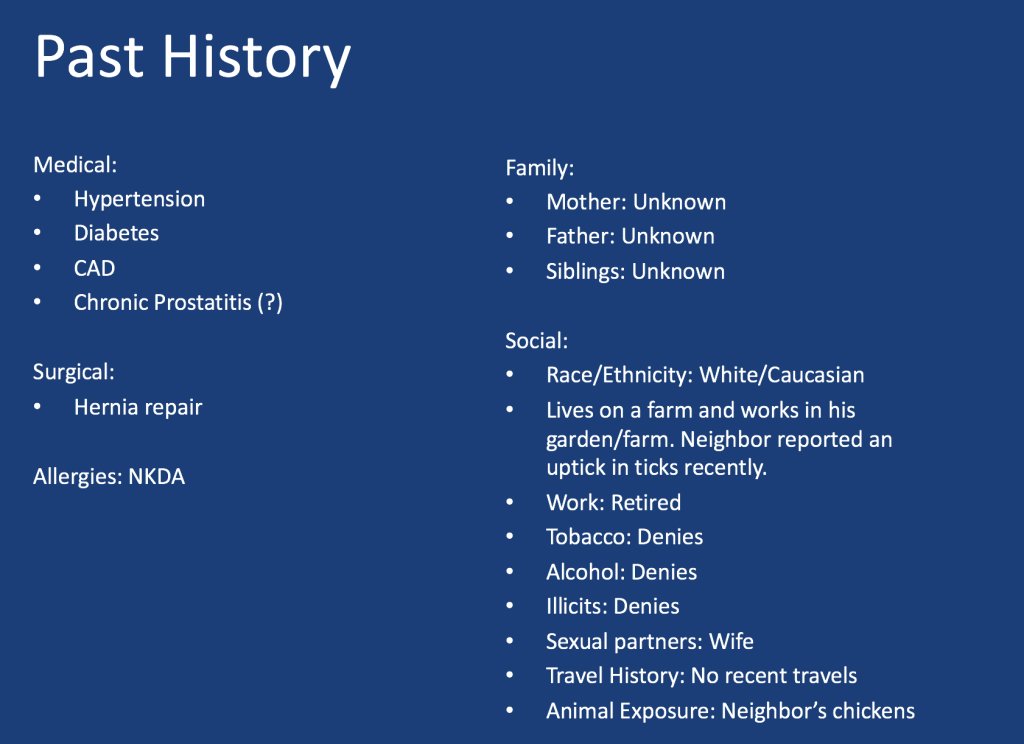
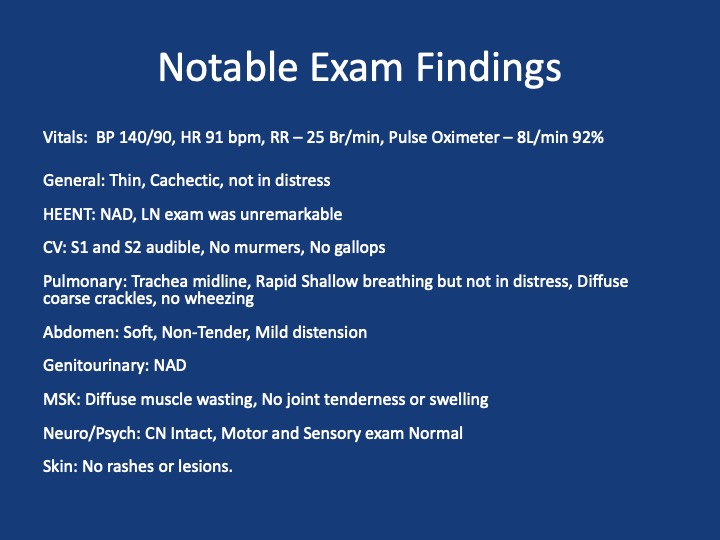
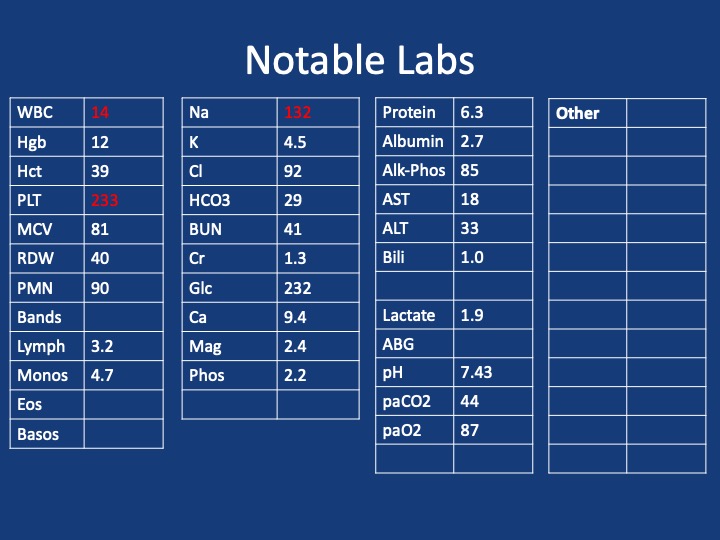
A male in her early 60s is transferred from a neighboring facility with a 1 week history of fatigue and lethargy. Three days prior to presentation he developed dyspnea and increased weakness with a near fall at home. HIs family also reported recent fevers, chills, dyspnea, and diarrhea. On his way to seek evaluation, he developed slurred speech without any other focal abnormalities.
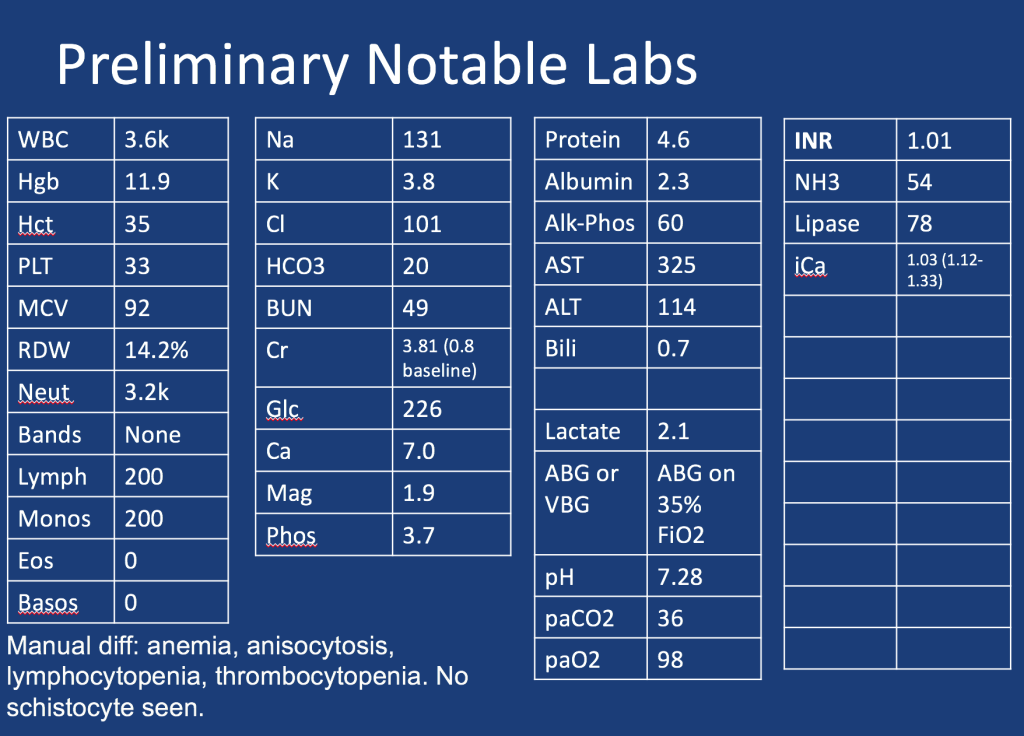
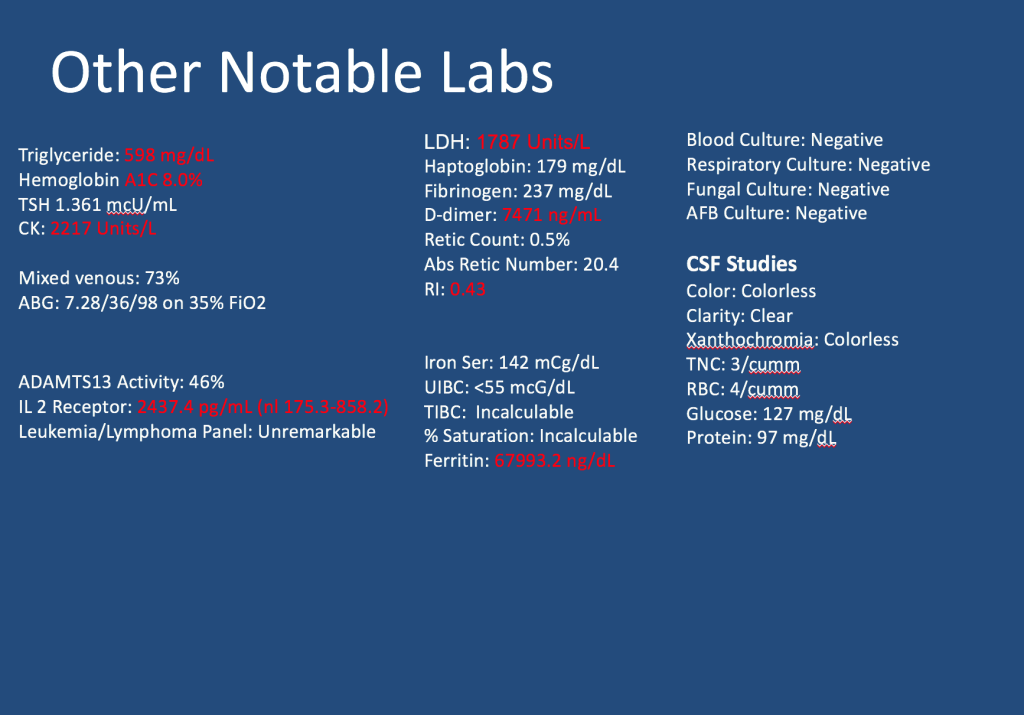
Additional information is summarized as below:
Follow along our episode to hear the final diagnosis and key teaching points from the case!
For “#RadiologyRounds” today, we won’t be looking at any imaging, but we’ll be looking at some vent wave forms and examining dysynchrony! This is a re-booted @david_furfaro Tweetorial. I hope you enjoy and this is an open invitation for all dysynchrony waveforms!
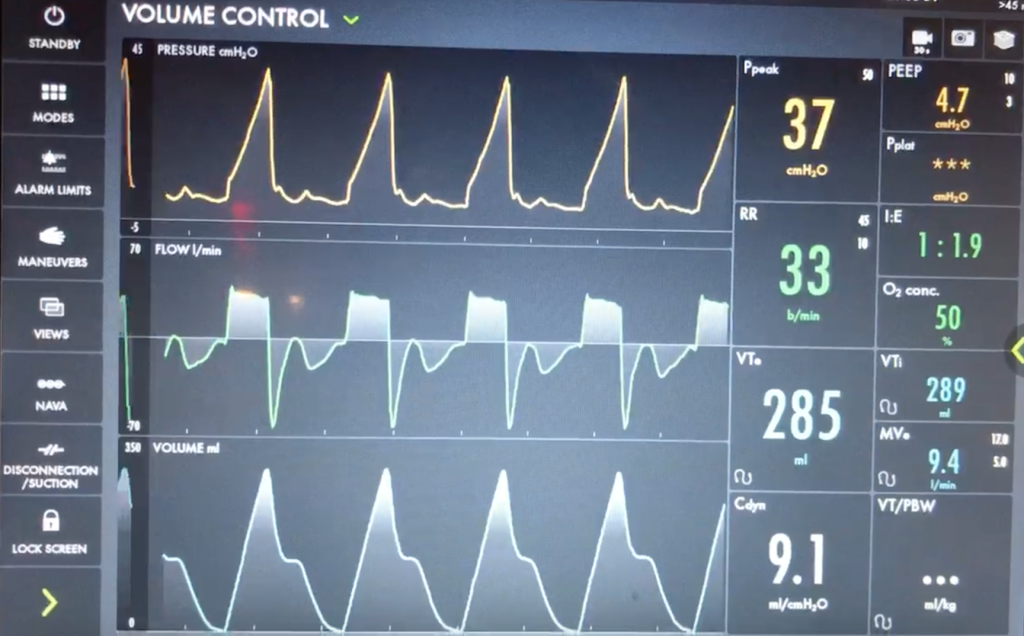
A 40s M is intubated for ARDS. In order to maintain lung protective ventilation, he was on high does of propofol, fentanyl and midazolam. His sedation is being weaned slightly now, and the RN calls for vent dysynchrony. His ventilator looks like this
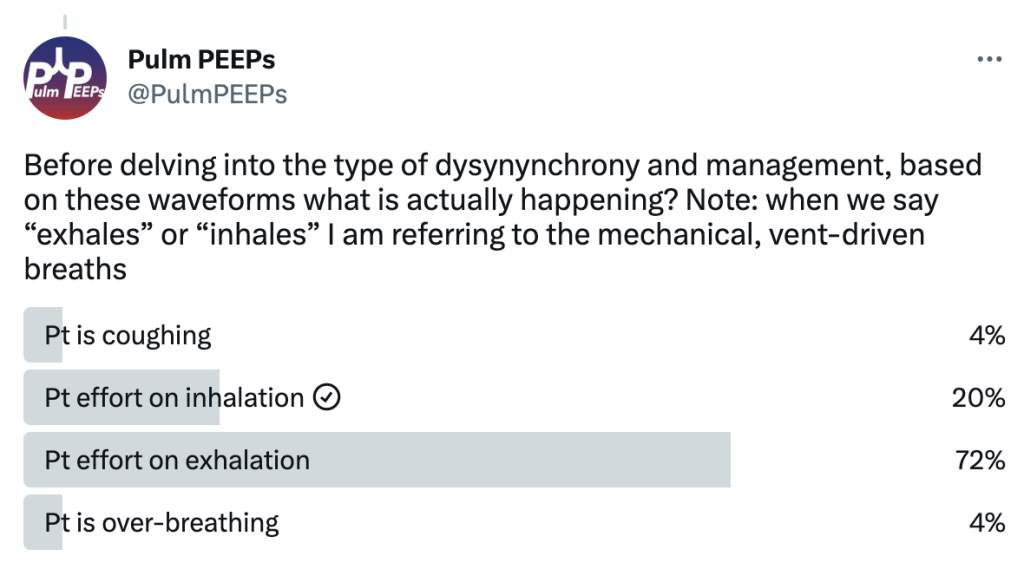
Before delving into the type of dysynynchrony and management, based on these waveforms what is actually happening? Note: when we say “exhales” or “inhales” I am referring to the mechanical, vent-driven breaths
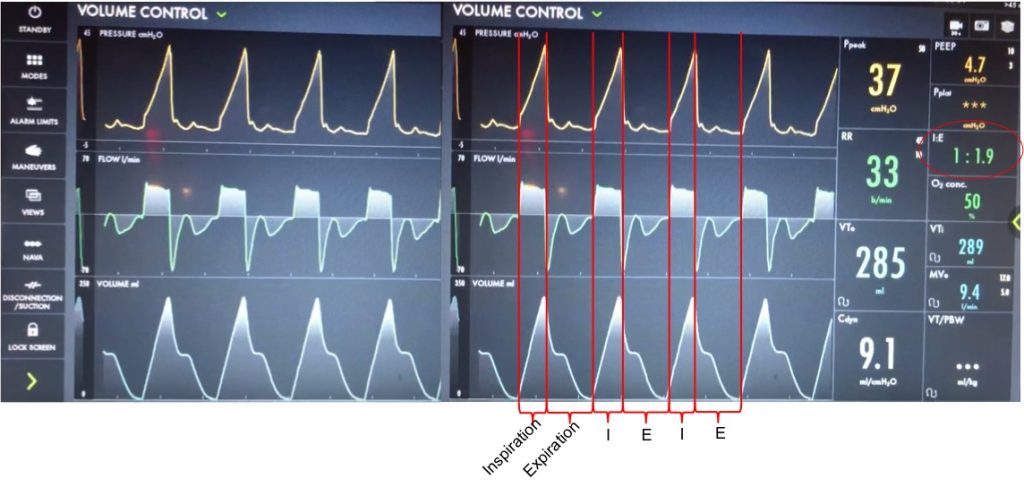
Let’s take a look at the waveforms and identify the phase of breathing. This is VC with a square flow waveform, so as a set volume is delivered, the flow is at a constant rate, and the pressure is measured. Expiration is about 2x as long as inspiration (determined by I time or flow rate)
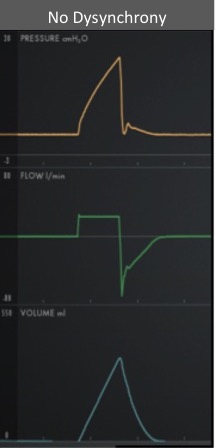
With a passive patient (no dysynchrony) after inspiration, the volume curve should show a smooth decrease with exhalation, the pressure curve should flatten to the set PEEP, and the flow will be negative and gradually return to 0 as the patient exhales
In our case, you can see simultaneous dysynchrony in all three waveforms during exhalation (red arrows) vs normal (orange lines). There is a pressure negative deflection; the flow quickly rises to 0 before returning to negative; and the volume curve plateaus as exhalation pauses
Putting this together, it means that during expiration there is an inspiratory effort. The patient is trying to inhale, which causes a negative pressure deflection, and a pause in air flowing out of the lungs. If this effort triggered a breath, there could be breath stacking. Notice that the same pattern occurs after every breath, and clinically we said the patient was still heavily sedated. This combination of findings is a type of dysynchrony called REVERSE TRIGGERING or ENTRAINMENT.
You could consider whether this dysynchrony was an ineffective effort, but the trigger sensitivity was low, and the pattern and consistent timing after inspiration is more consistent with reverse triggering.
The change in pressure and flow of a ventilator-initiated, mandatory breath stimulates an inspiratory effort from the patient. Theories differ on if this is mediated by the diaphragm or central respiratory center. This can start during the ventilator-delivered breath, or afterwards in exhalation, as with our patient.
Reverse triggering often occurs in heavily sedated patients, and is defined by a stable, repetitive pattern (i.e. it is not voluntary, but reflex mediated). It can also occur in anoxic brain injury. Treating it involves breaking the pattern and avoiding harmful therapies. It can even be induced in healthy patients but this is much less clinically relevant, and is rare.
DO NOT just increase the trigger sensitivity of the vent. This can stop breath stacking but does not prevent dysynchrony and it can cause harmful changes in transpulmonary pressure. For this patient, sedation was lightened slightly, and the respiratory rate decreased and the pattern of reverse triggering ultimately broke without the need for paralysis.
Join us as we head to the Texas Medical Center and are joined by Dr. Bitar and Dr. Gotur from Houston Methodist Pulmonary and Critical Care Medicine.
Meet our Guests
Dr. Mohamad Bitar is a Pulmonary and Critical Care Fellow at the Houston Methodist Pulmonary and Critical Care Program in Houston, Texas. Dr. Bitar completed his medical school at Misr University for Science and Technology and his Internal Medicine residency at Good Samaritan Hospital.
Dr. Deepa Gotur is an Associate Professor of Clinical Medicine at Weill Cornell Medical College and an Adjunct Associate professor at Texas A&M. She is also the Pulmonary and Critical Care Program Director at Houston Methodist. She is a sepsis and ARDS researcher, as well as a dedicated educator.
Case Presentation
A 40s-year-old male presents with 3 months of progressive shortness of breath. He was diagnosed with COVID and given treatment with steroids, and antibiotics with no response.
He presented to the hospital 3 months later after not being able to carry out daily activities and was found to have low oxygen saturation
Admitted, initial CT Chest – showed “Non-specific patchy ground-glass bilateral pulmonary infiltrates with Coarsened interstitial markings that could be related to COVID-19/atypical infection”
References and further reading
1. Silva, C. Isabela S. MD, PhD; Müller, Nestor L. MD, PhD. Idiopathic Interstitial Pneumonias. Journal of Thoracic Imaging 24(4):p 260-273, November 2009.
2.Gruden JF, Naidich DP, Machnicki SC, Cohen SL, Girvin F, Raoof S. An Algorithmic Approach to the Interpretation of Diffuse Lung Disease on Chest CT Imaging: A Theory of Almost Everything. Chest. 2020 Mar;157(3):612-635.
3. Ryu JH, Daniels CE, Hartman TE, Yi ES. Diagnosis of interstitial lung diseases. Mayo Clin Proc. 2007 Aug;82(8):976-86.
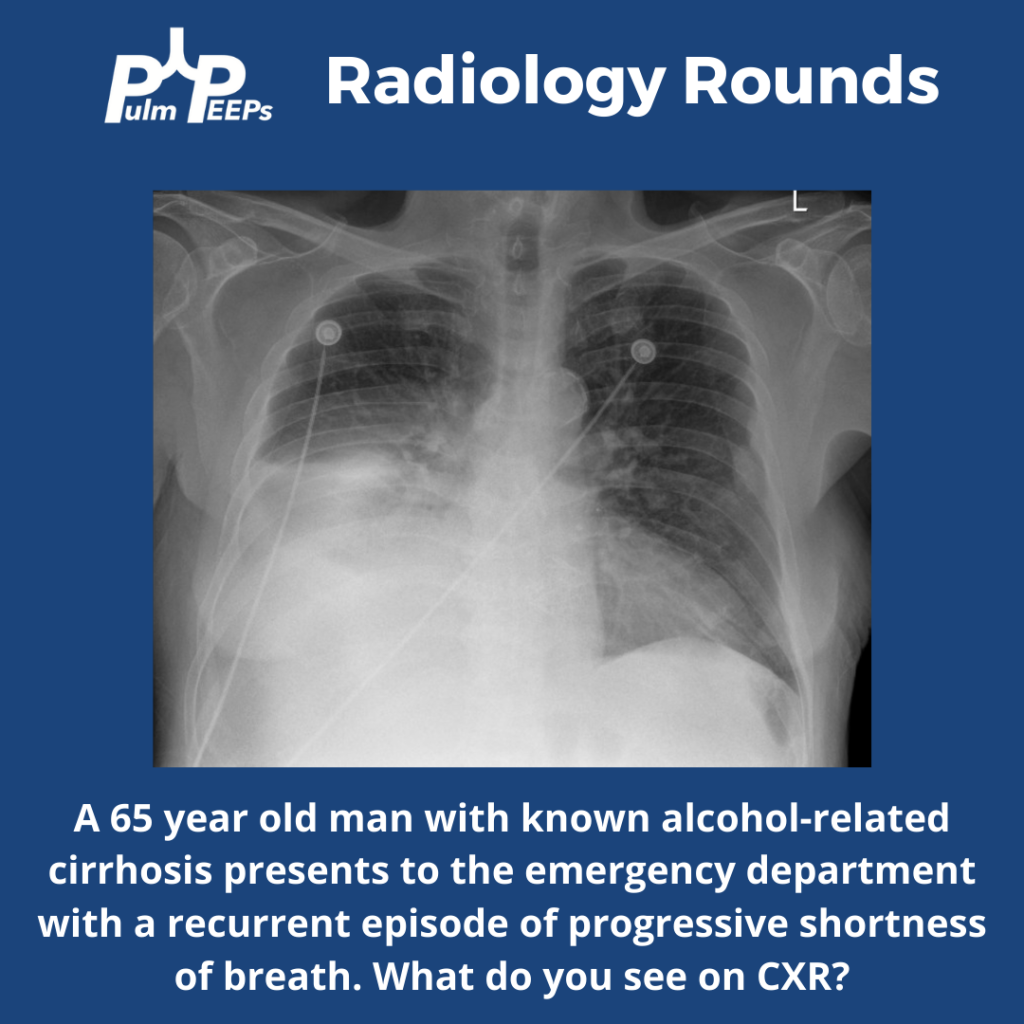
It is Tuesday #RadiologyRounds time! We are in a pleural state of mind here at Pulm PEEPs. This is another great case authored by rockstar-associate editor @TessLitchman
A 65-year-old man with cirrhosis presents to the ED with progressive shortness of breath:
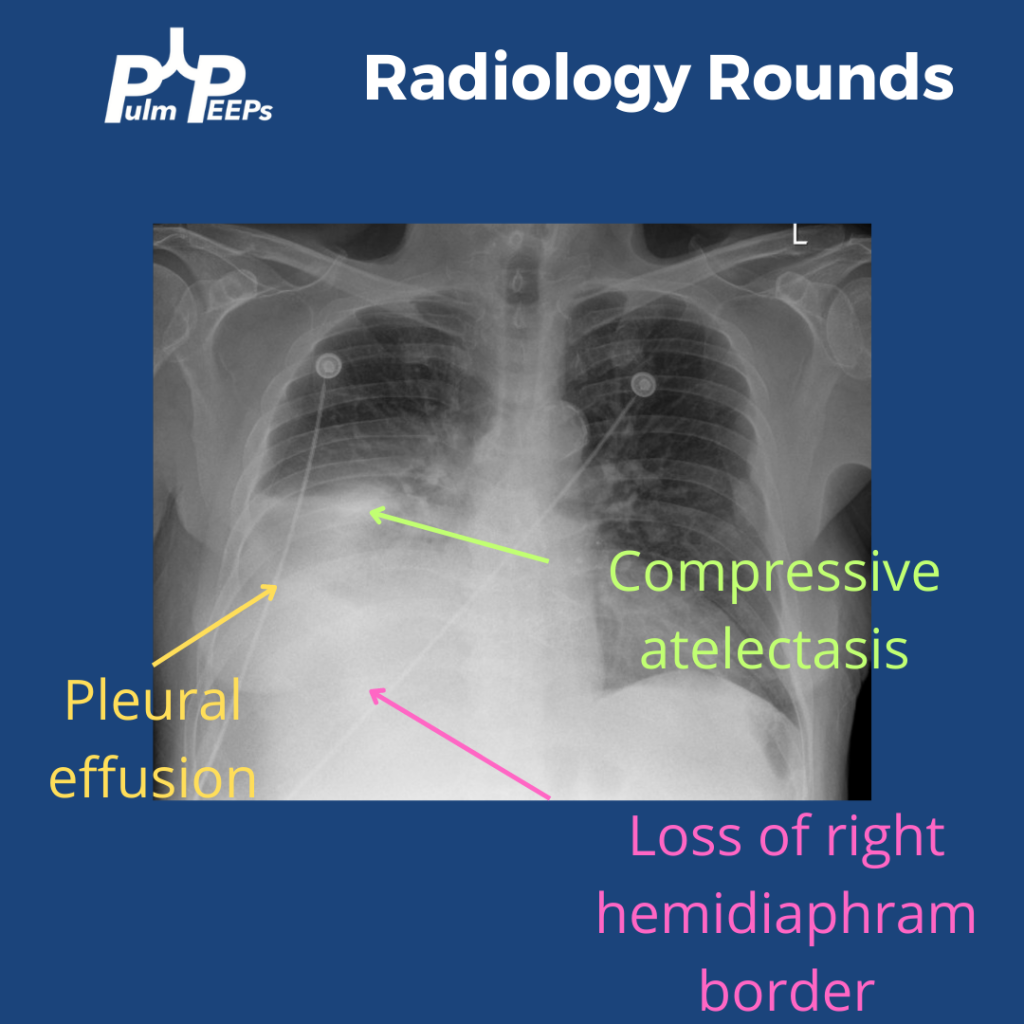
The CXR has a right lower opacity decreasing in density that is silhouetting the right hemi-diaphragm without signs of volume loss on the right concerning for pleural effusion. There is also associated atelectasis adjacent to the effusion
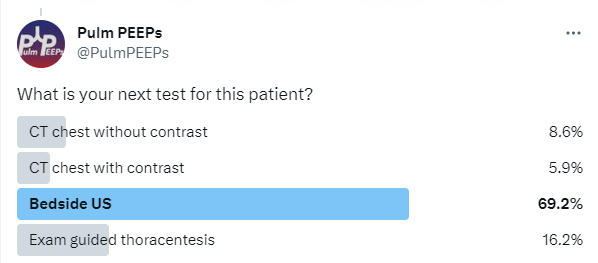
What is your next step for this patient?
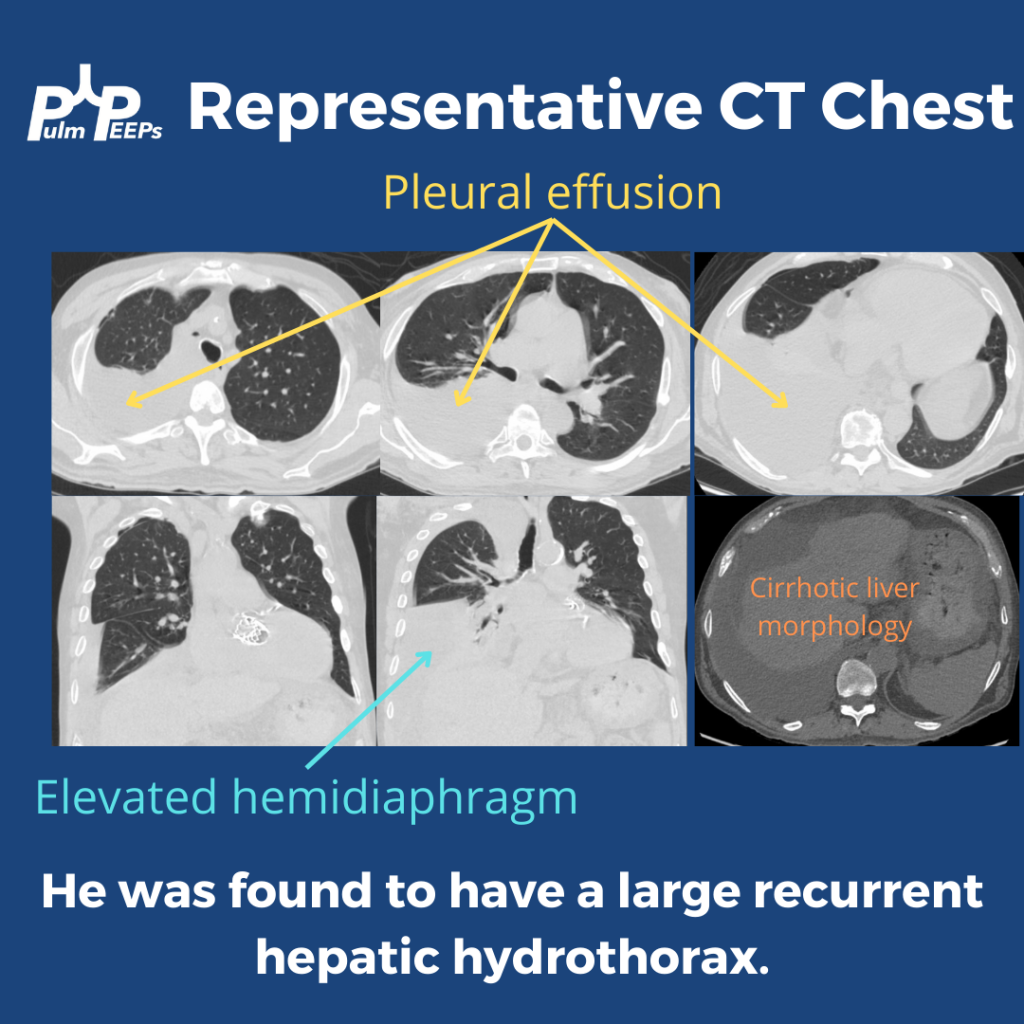
This patient had a bedside POCUS revealing a simple pleural effusion and abdominal ascites. He also had a CT scan performed:
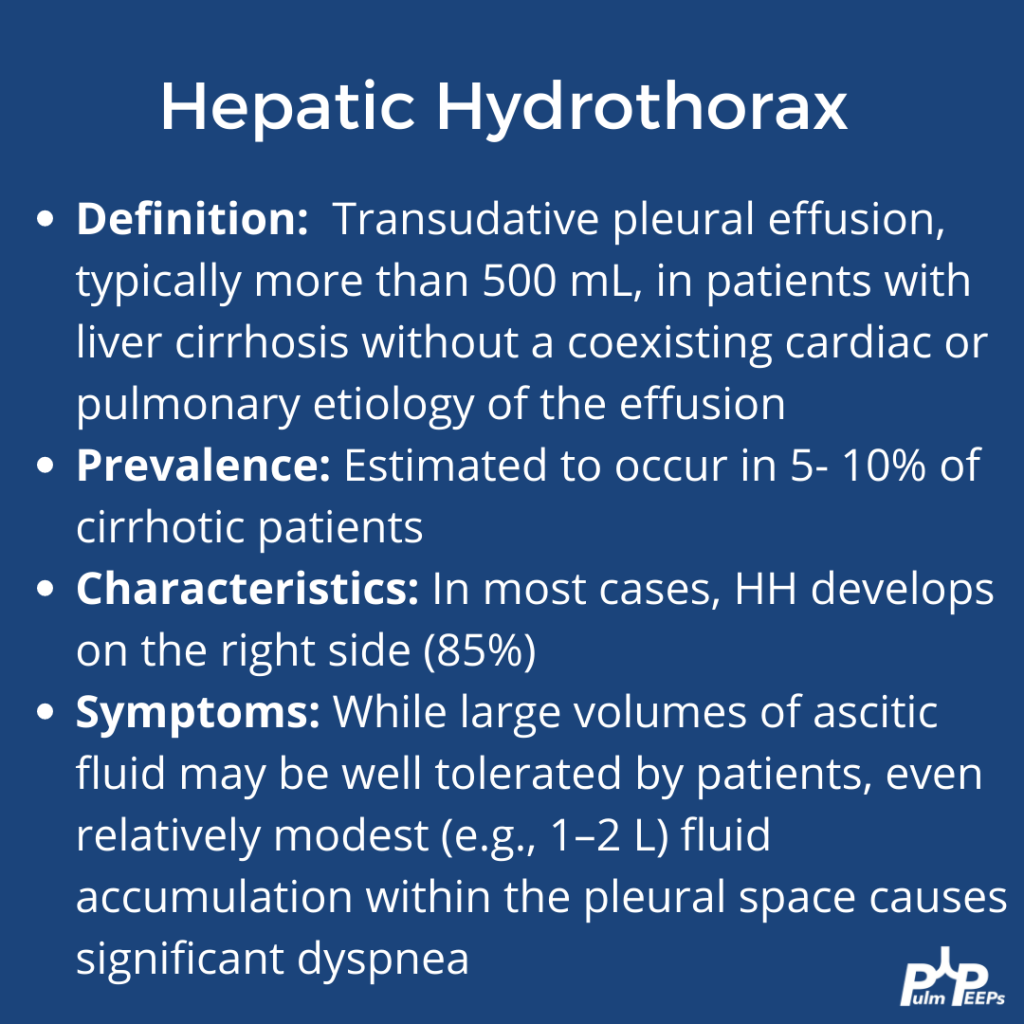
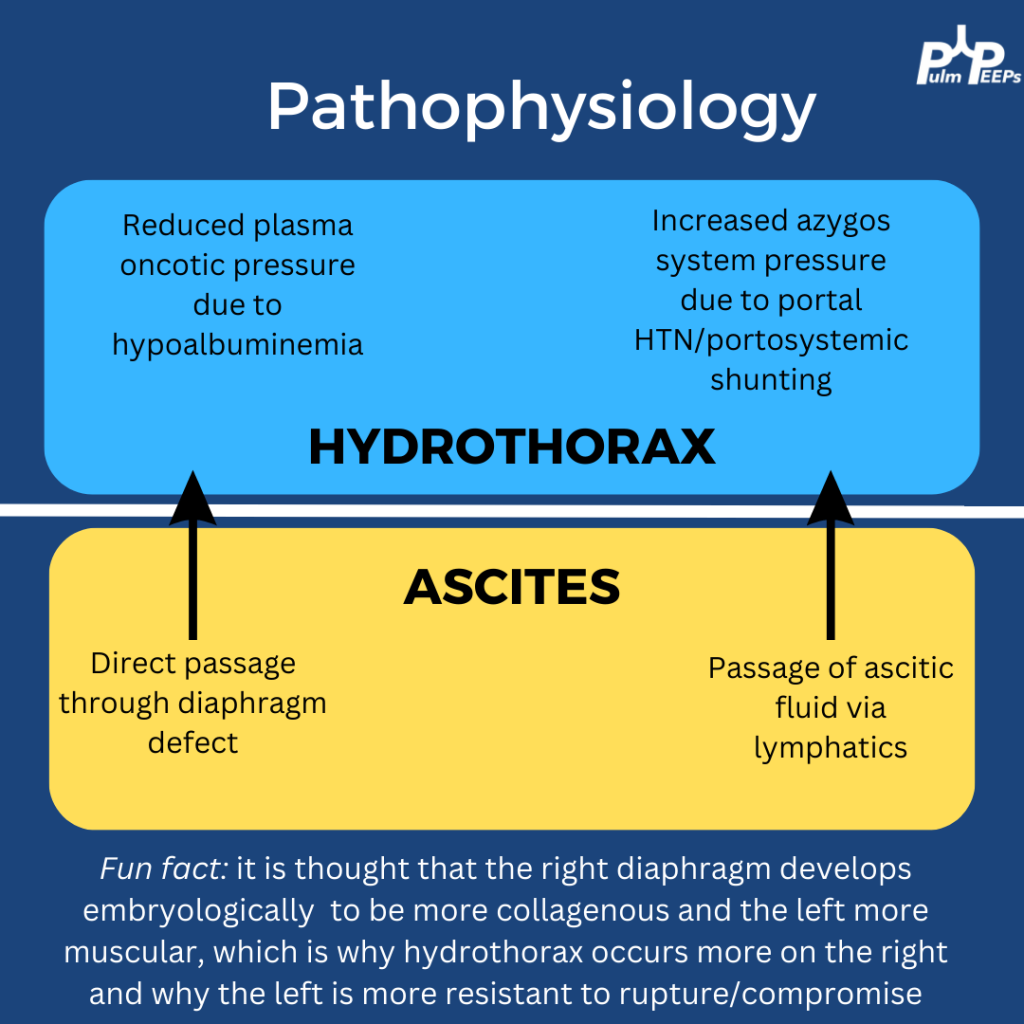
Based on his imaging and history, the most likely diagnosis on the differential was a hepatic hydrothorax. Here is some more information on hepatic hydrothoraces:
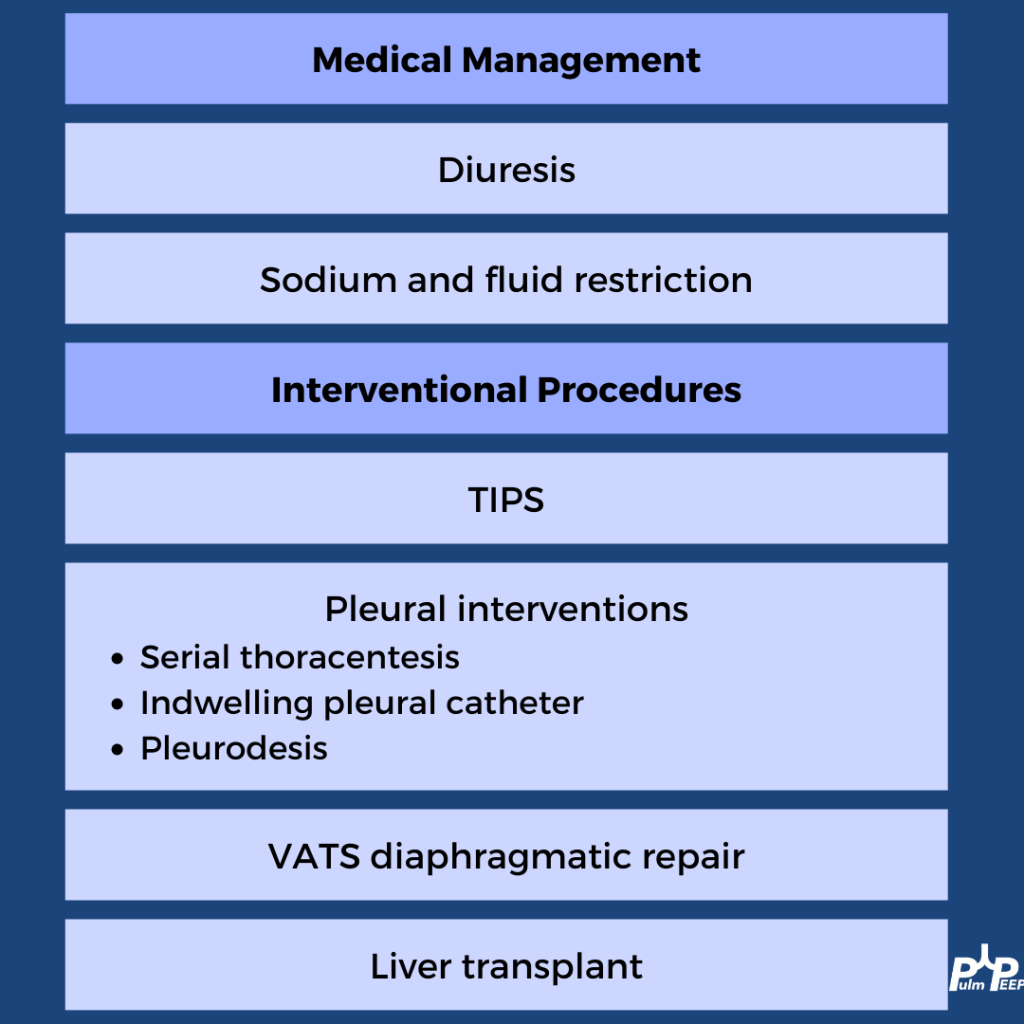
A transudative effusion was confirmed on thoracentesis, and no other clear etiologies were identified The treatment of hepatic hydrothorax should always start with medical management of volume overload in cirrhosis. Pleural procedures can be used for disease that is refractory
We continue our Top Consult Series on Pleural Disease and bring you a dedicated episode on Parapneumonic effusions. We are joined by two guest experts, Dr. David Feller-Kopman and Dr. Mihir Parikh. Listen in as we discuss the spectrum of parapneumonic effusions, including simple parapneumonic effusions, complicated parapneumonic effusions, and empyema. You will hear what to look for on imaging, what tests to send with pleural drainage as well as discuss the need for surgical consultation.
Meet our Guests
Dr. Mihir Parikh is currently an Assistant Professor of Medicine and academic interventional pulmonologist at Beth Israel Deaconess Medical Center. He is a highly esteemed educator and has worked to incorporate simulation training to improve procedural training for trainees and is a master of pleural disease.
Dr. David Feller-Kopman is a Professor of Medicine and the Section Chief of Pulmonary and Critical Care Medicine at Darmouth whose clinical and research expertise span the field of interventional pulmonology. Dr. Feller-Kopman is a true master of pleural disease, and has authored more than 225 peer-reviewed manuscripts and has been a leader for both ATS and CHEST committees.
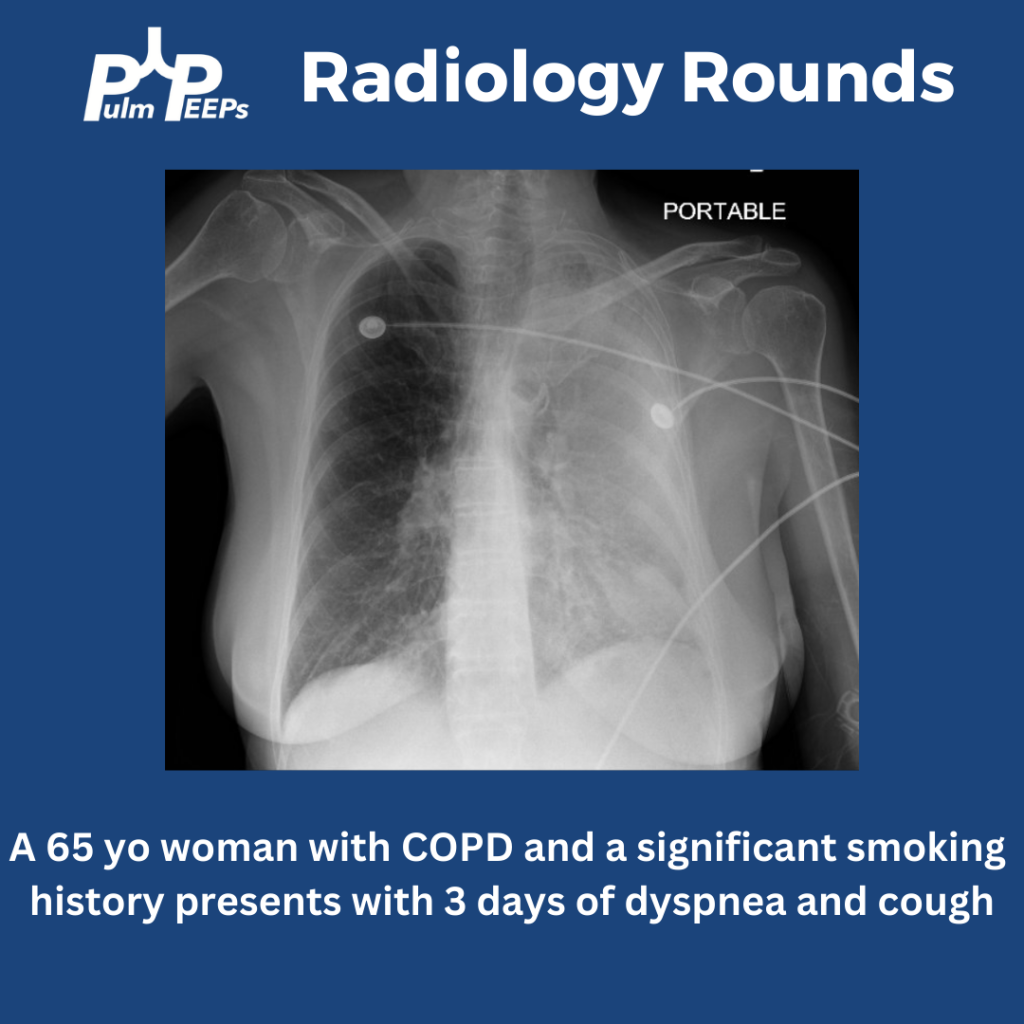
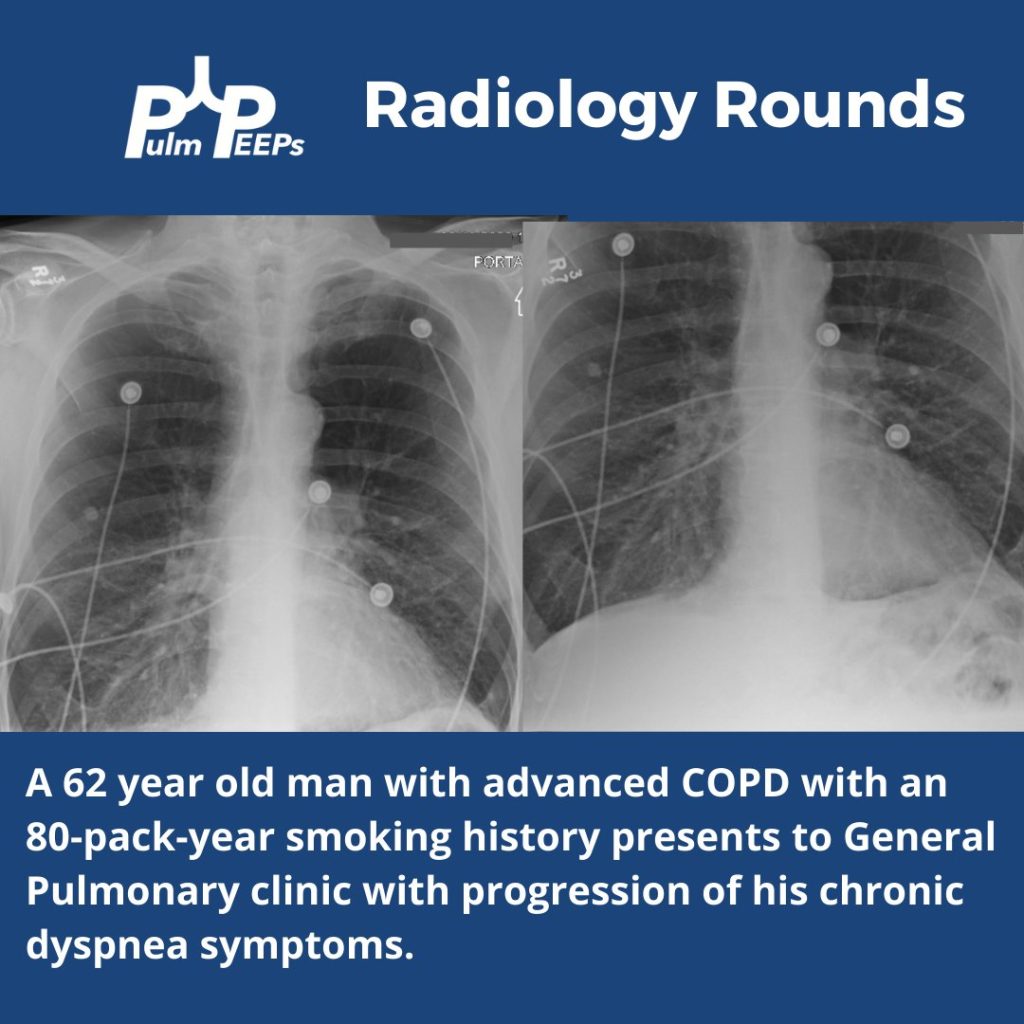
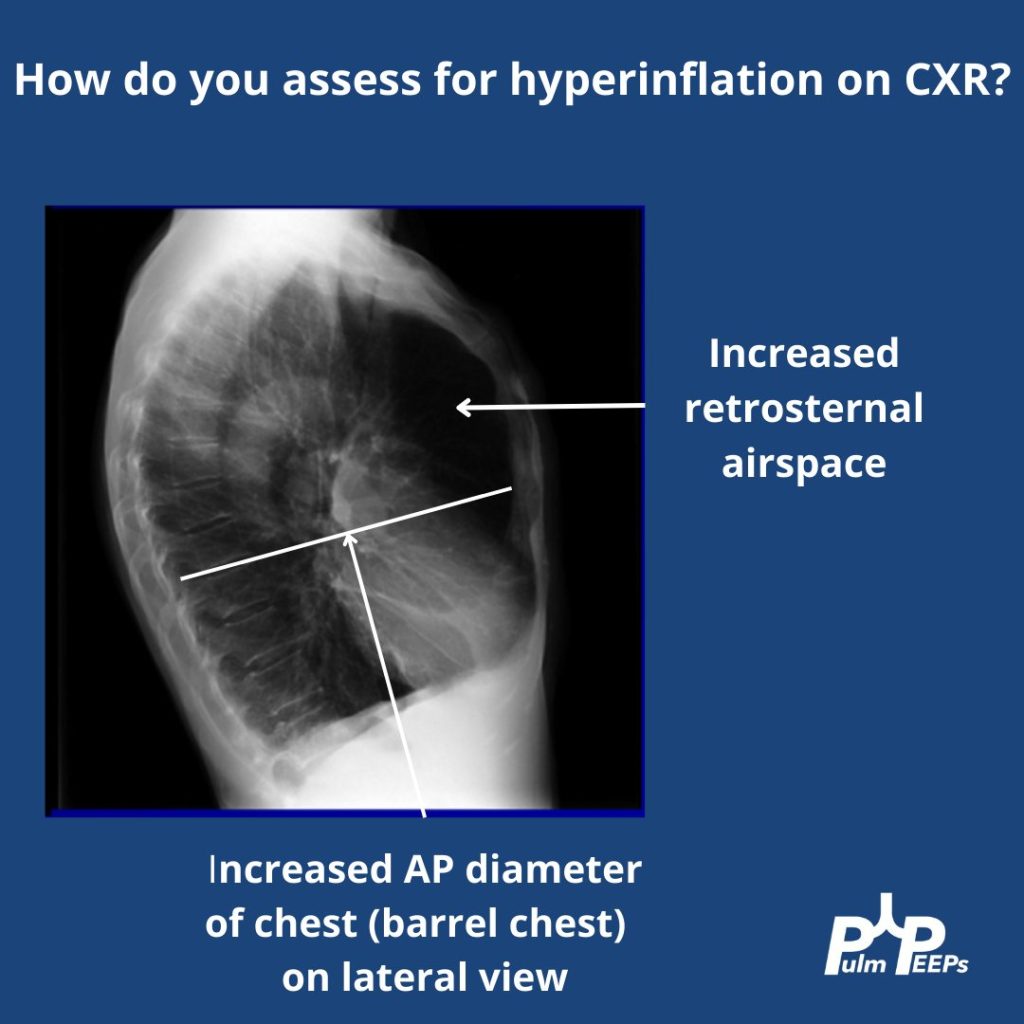
A portable film is obtained on a 65 yo woman with COPD presenting with progressive dyspnea and cough.
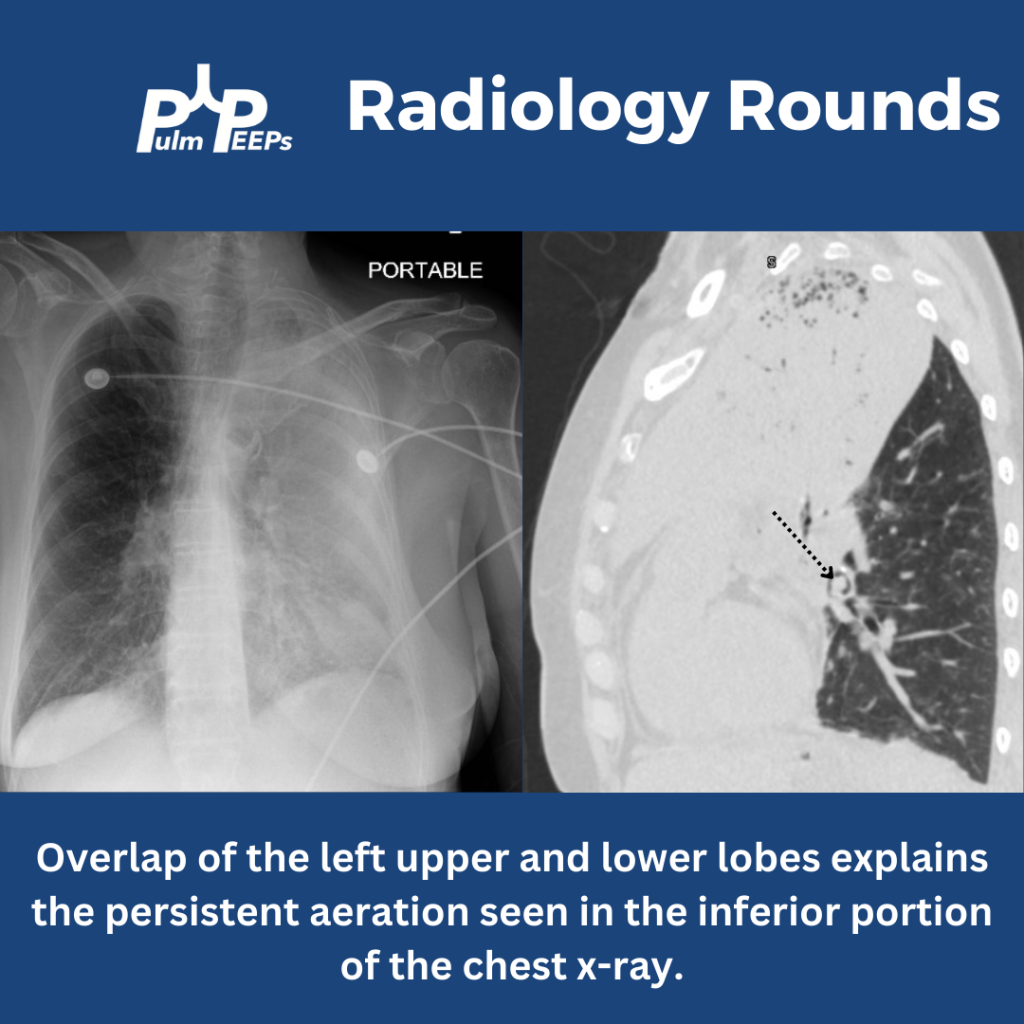
The image shows near complete opacification of the left lung. There is no ipsilateral or contralateral tracheal deviation which you would expect with atelectasis or a large pleural effusion, respectively. A CT chest is obtained to better visualize the parenchyma.
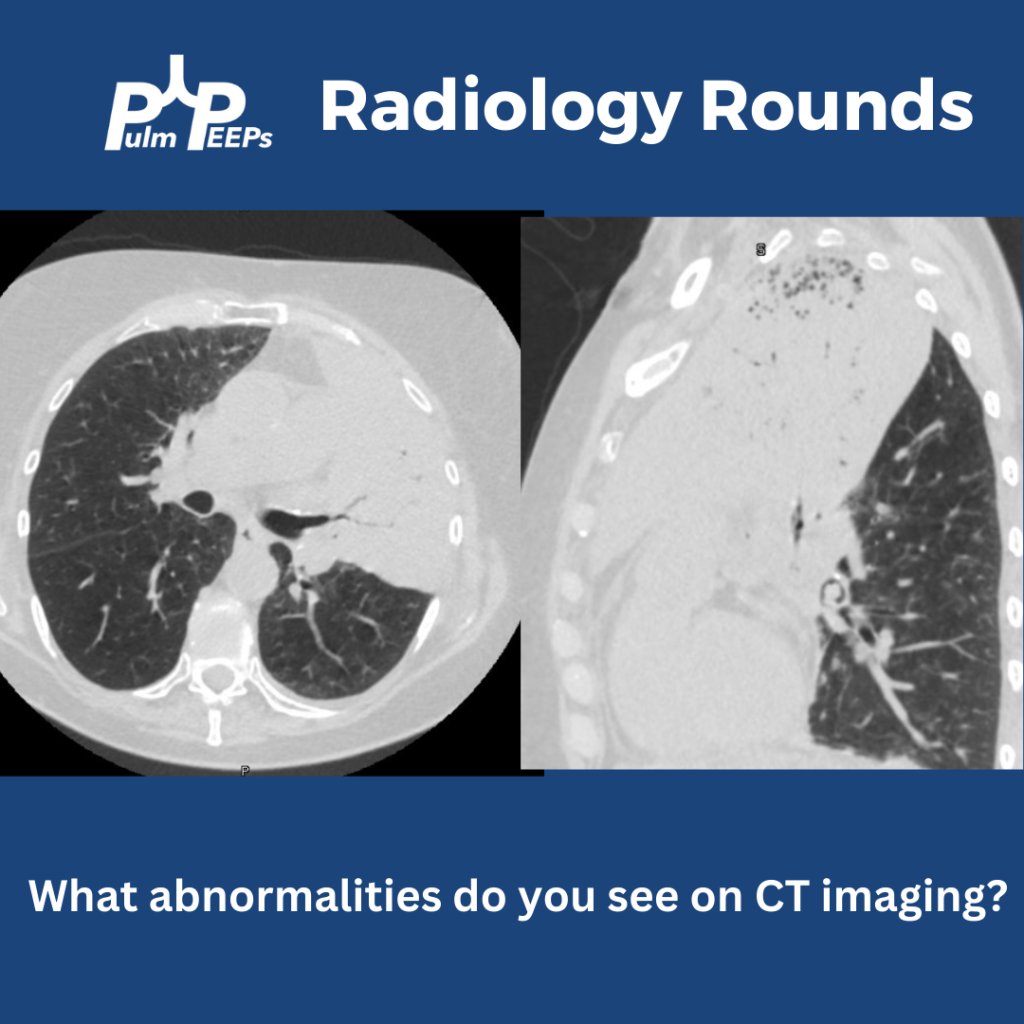
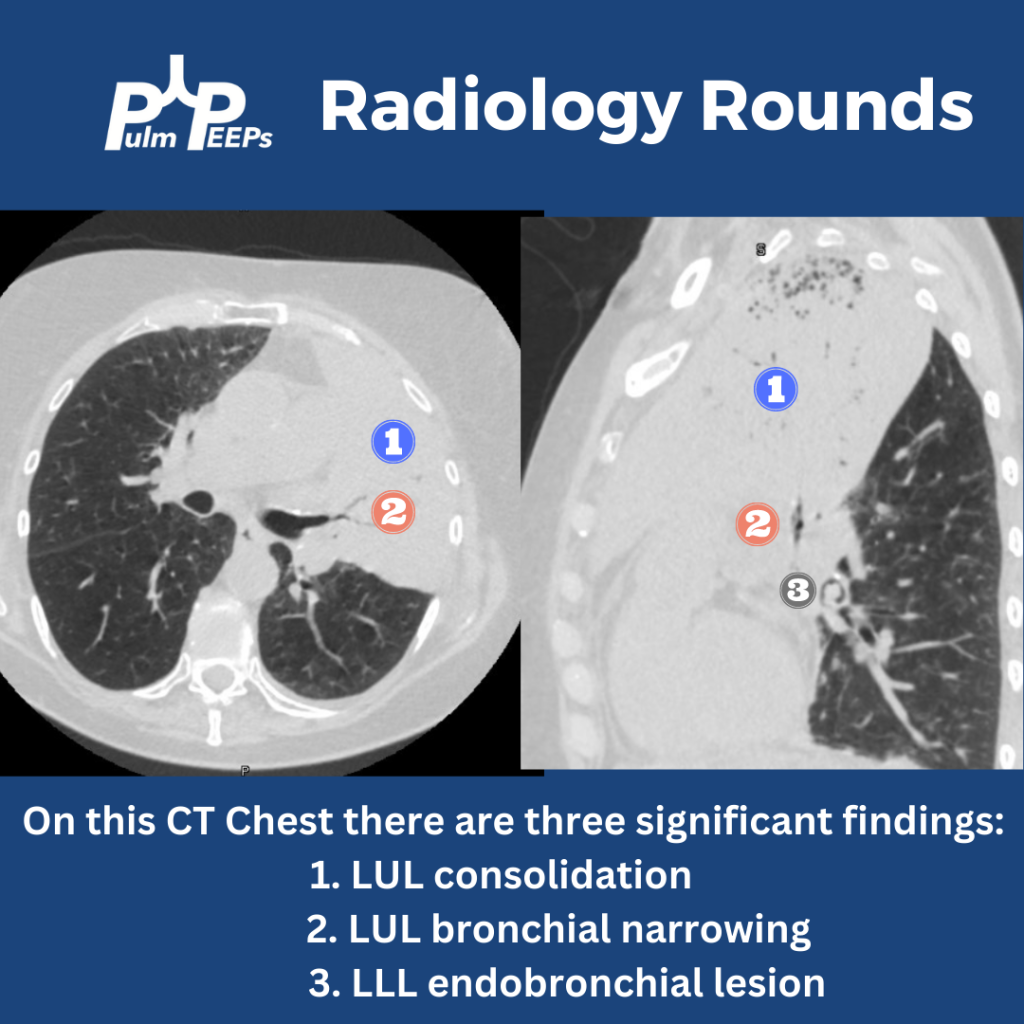
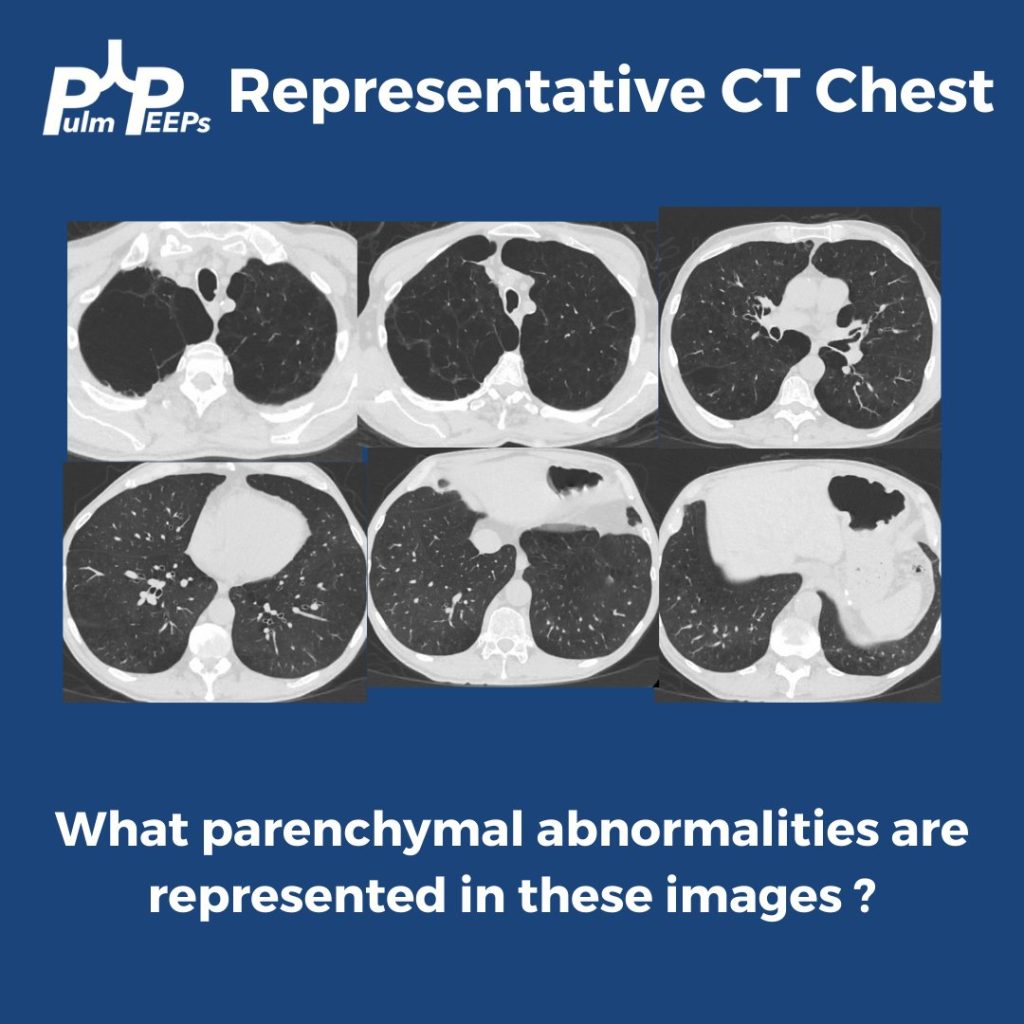
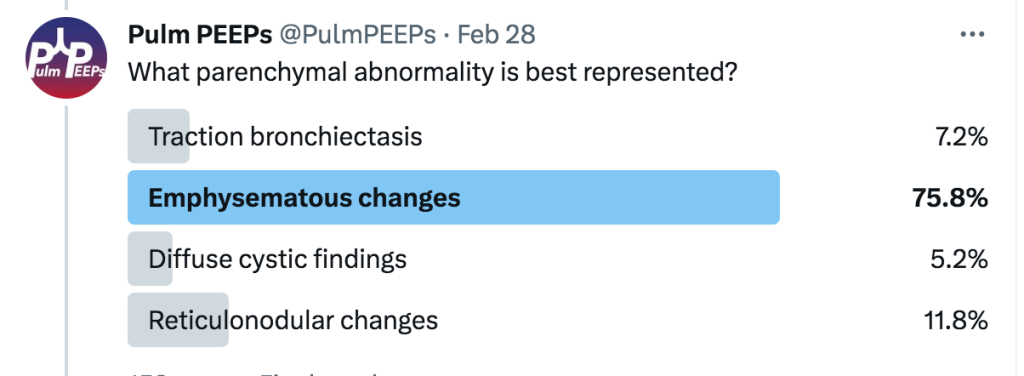
The CT chest shows all three findings as noted below.
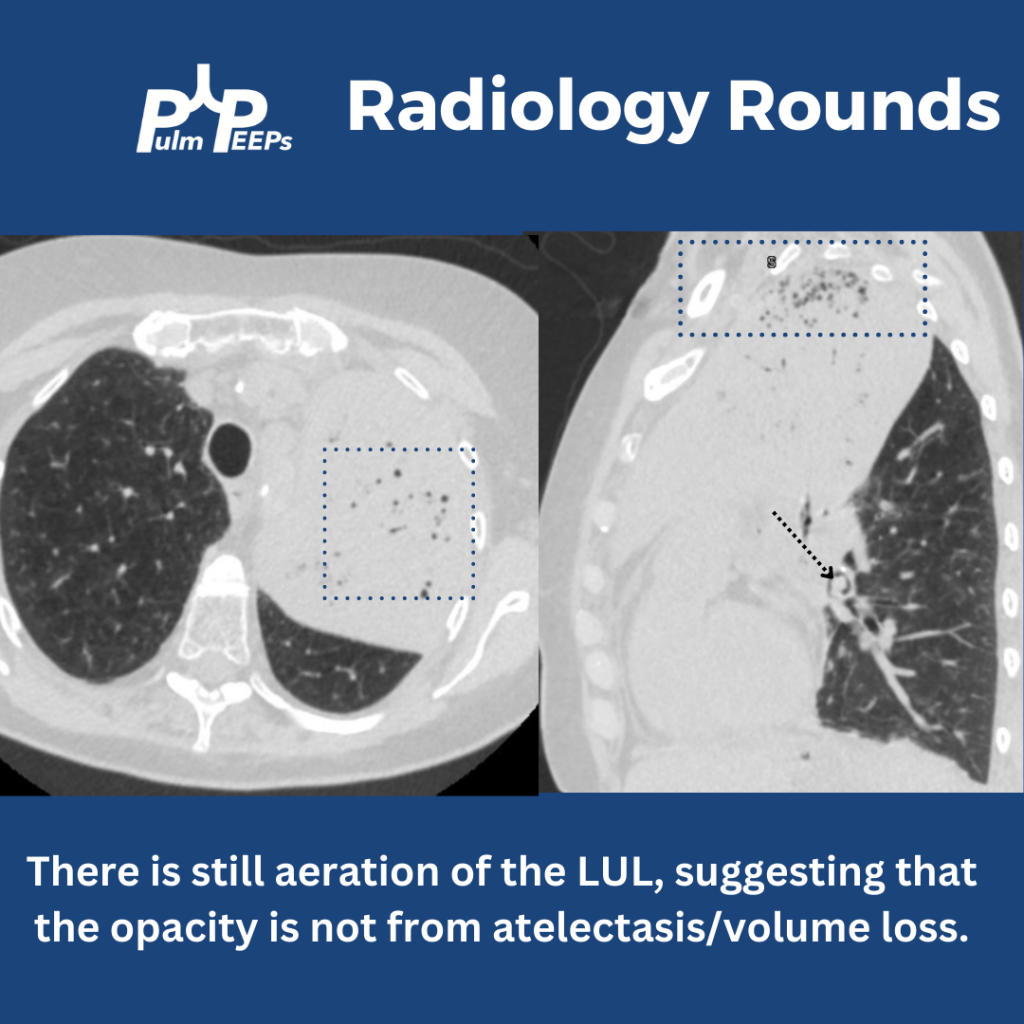
Yes! There is still aeration in some of the upper lobe, which would not be the case if this were caused by profound atelectasis. Also, atelectasis of such a large territory of the lung would usually cause traction on surrounding structures.
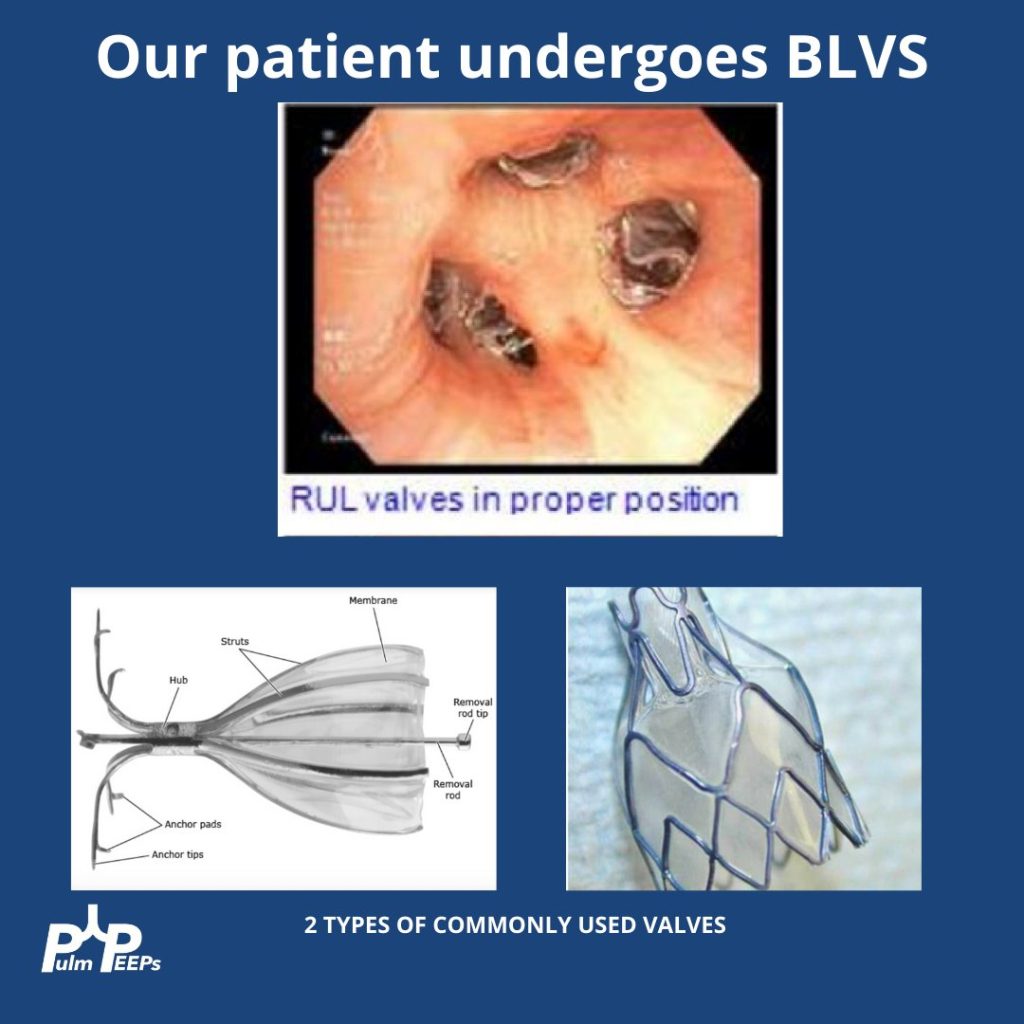
Having seen the CT, can you explain why the x-ray showed aeration in the inferior, left hemithorax? This is from the overlap of the left upper and lower lobes when viewed anteriorly. The sagittal view of the CT demonstrates this nicely.
Today the PulmPEEPs are joined by two amazing educators as we start off our Top Consult series on Pleural Disease. Join us today as we go through cases to learn a systematic approach for evaluation and management of pleural effusions.
Meet our Guests
Dr. Mira John received her medical degree from Tulane University School of Medicine in New Orleans and completed internal medicine residency at Icahn School of Medicine at Mount Sinai. She is currently a second-year pulmonary and critical fellow at the University of Washington.
Dr. Ylinne Lynch completed her fellowship training at the University of Washington and is currently a Clinical Instructor at the UW. She is a great medical educator and spends her clinical time on the pulmonary consult service as well as in the ICU.
We are extremely excited for another PulmPEEPs Roundtable table discussion today. We have spent multiple episodes talking about different aspects of ARDS and respiratory failure. Today, multiple expert guests return, as well as a new guest to the show, to discuss the future of ARDS research. This is a can’t miss discussion that is so jam-packed with pearls you’ll have to listen twice!
Meet Our Guests
Carolyn Calfee is a Professor of Medicine and Anesthesia at the University of California, San Francisco. She is a world-renowned ARDS researcher and has authored multiple landmark studies in the field. She previously joined us for a discussion on ARDS precision medicine and phenotypes.
Ewan Goligher is an Assistant Professor at the University of Toronto and University Health Network. He has published many practice-changing papers in ARDS. These have included prospective studies and some fantastic retrospective analyses that have fundamentally shaped our interpretation of trial results. He previously came on the show discussing lung and diaphragm protection.
Sarina Sahetya is an Assistant Professor of Medicine at Johns Hopkins. She is a funded researcher in ARDS and respiratory physiology and has published multiple studies on lung protection and ARDS. She last helped us understand how to titrate PEEP in ARDS.
Matthew Semler is an Assistant Professor of Medicine and Biomedical Informatics at Vanderbilt University Medical Center, where he is also the Associate MICU Director and the co-director of the Inpatient Division of the Learning Healthcare System at Vanderbilt. Through his role as Chair of the Steering Committee for the Pragmatic Critical Care Research Group, he has helped lead more than two dozen randomized trials leading to multiple high-impact publications.