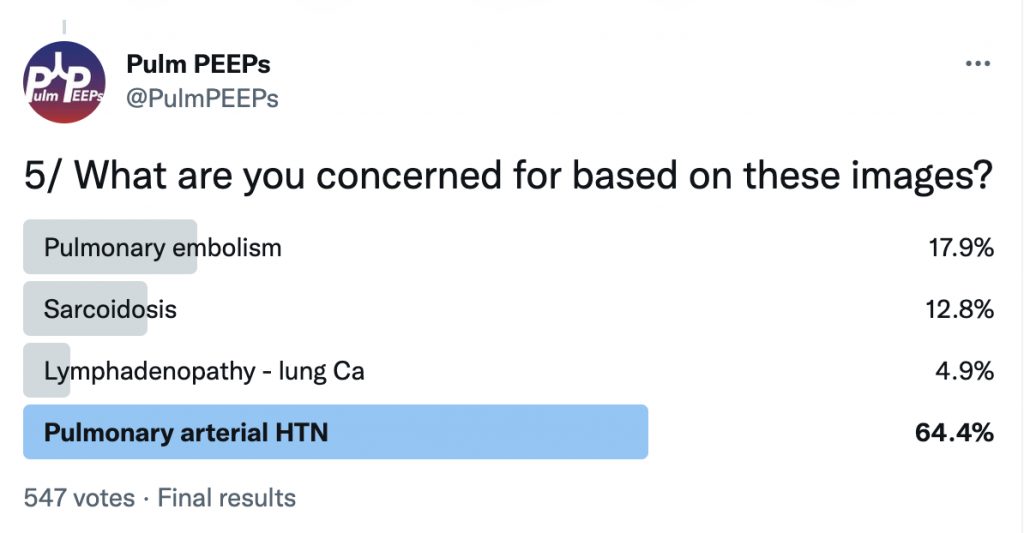
For Radiology Rounds this week we’ll be looking at multiple imaging modalities to help solve the case. Please follow along on Twitter for our live polls and for ongoing discussion of the case.
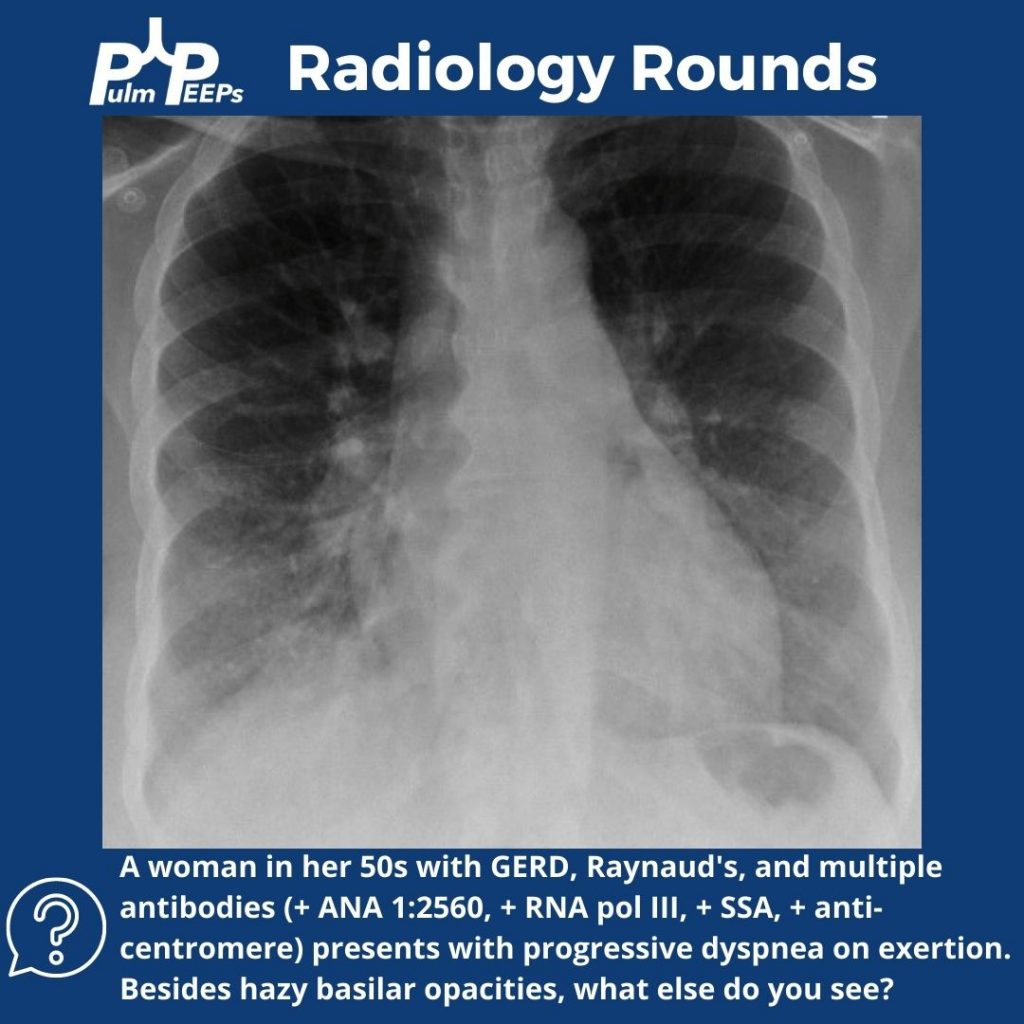
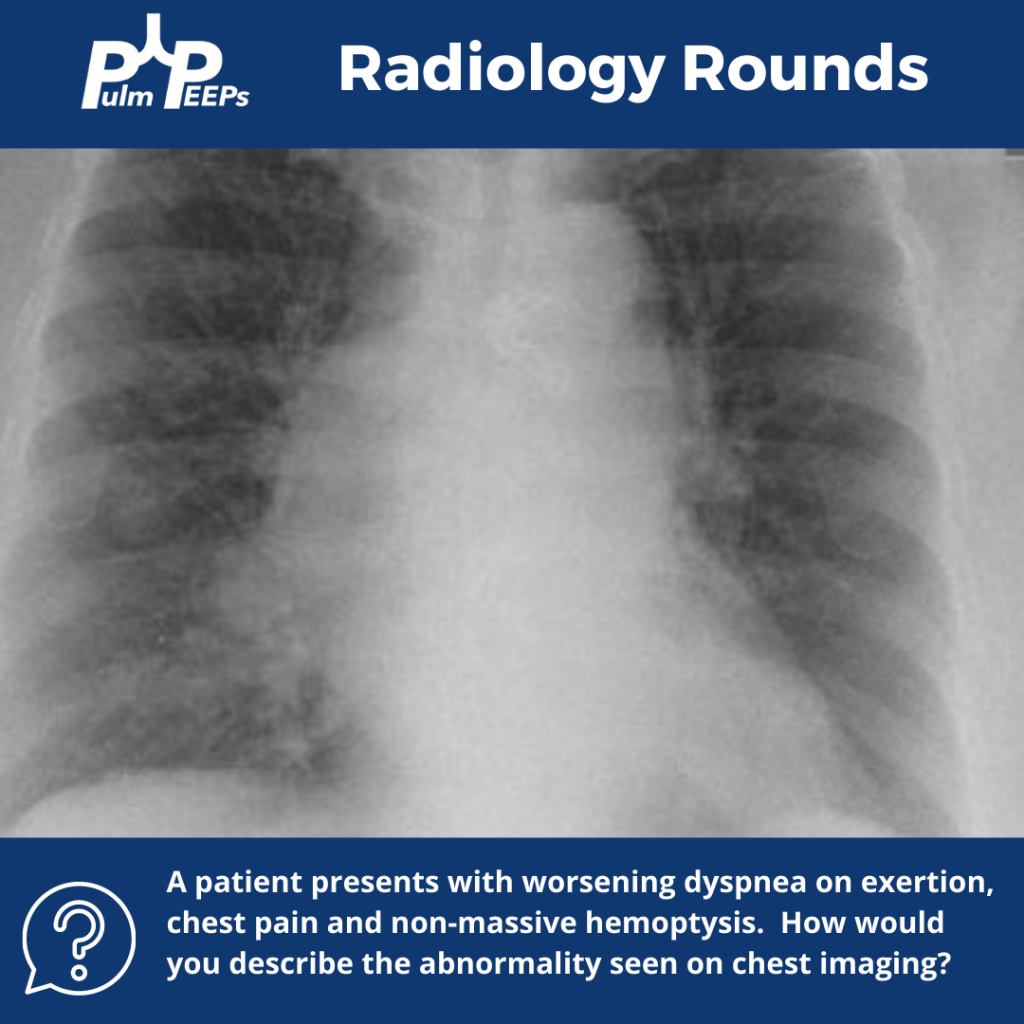
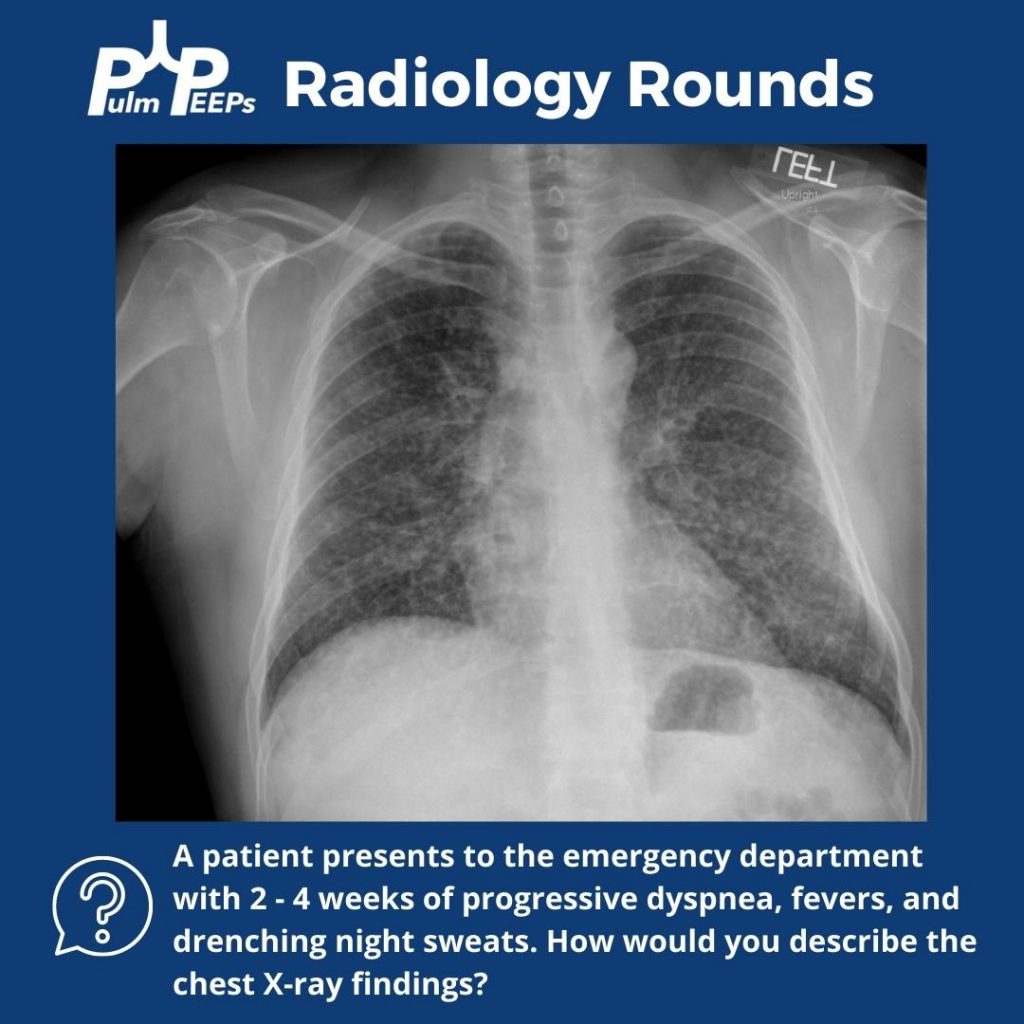
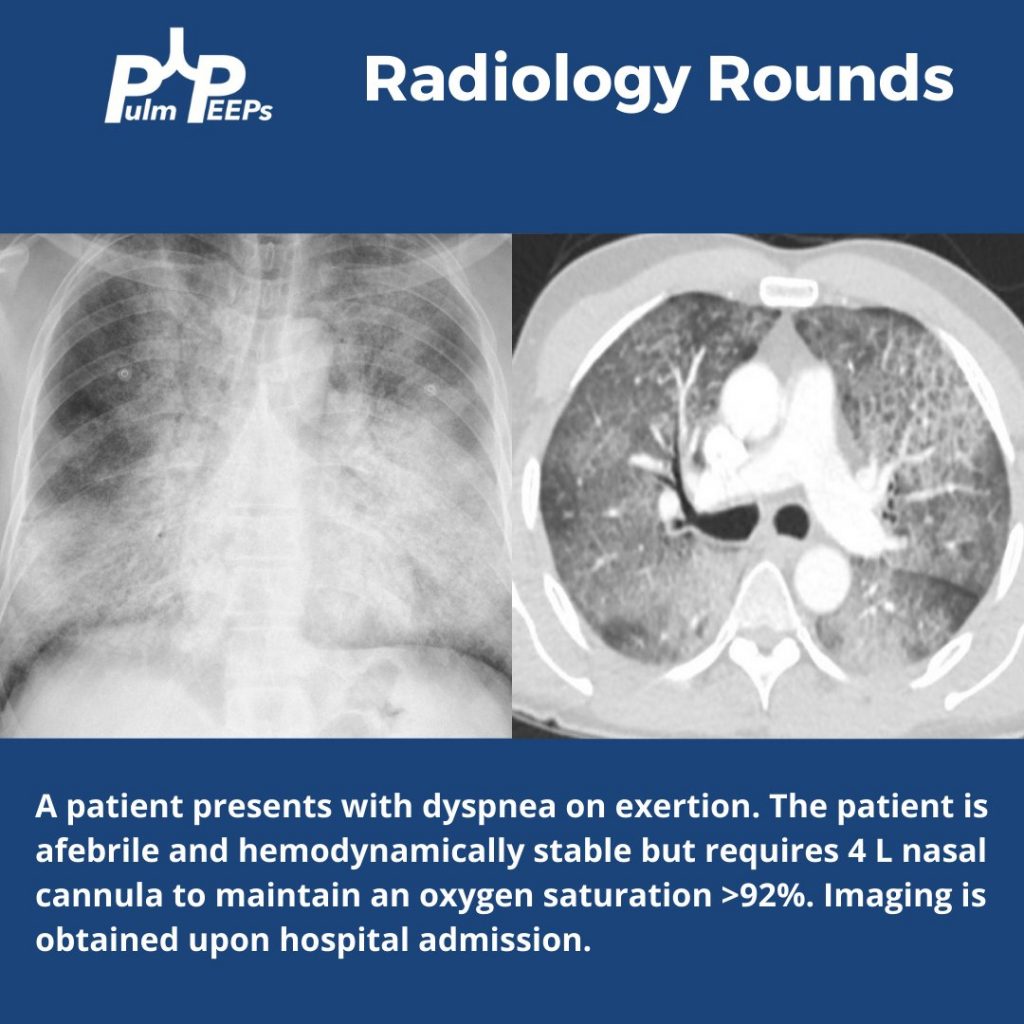
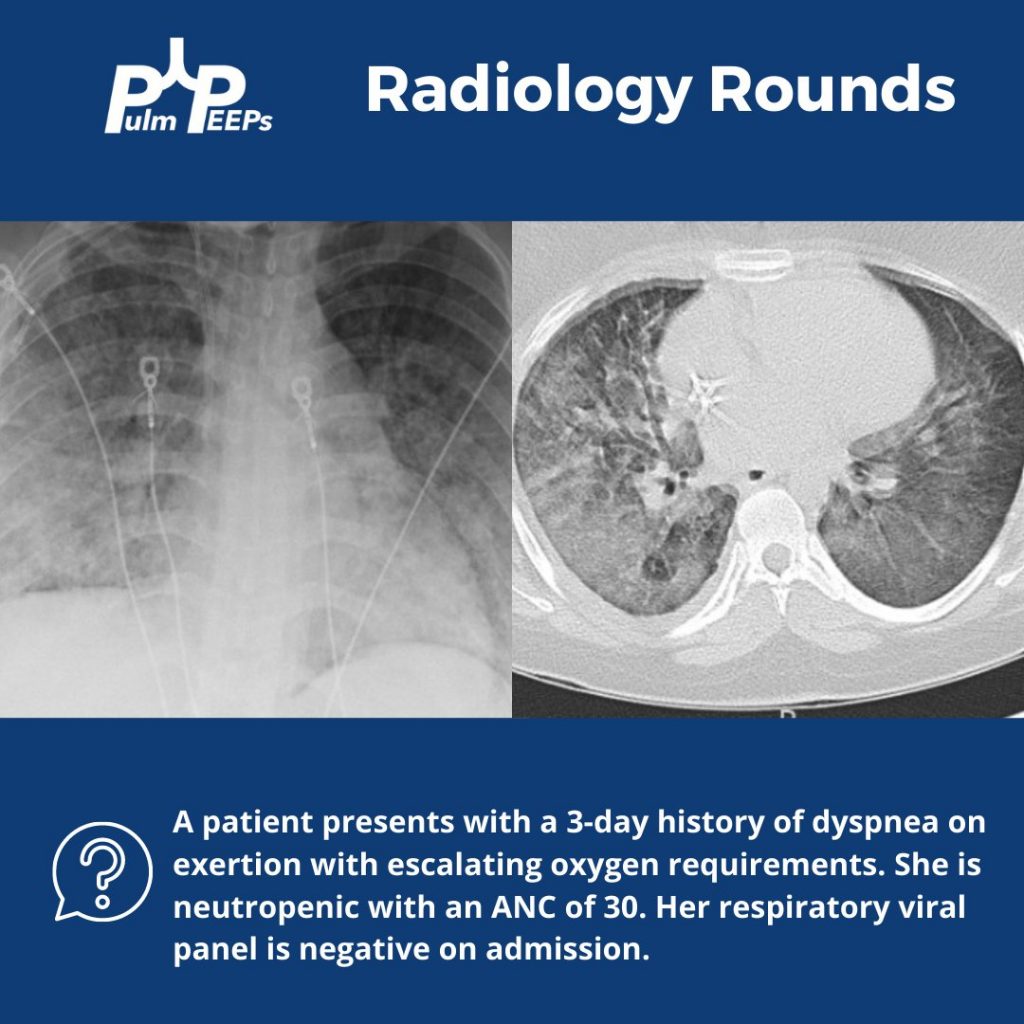
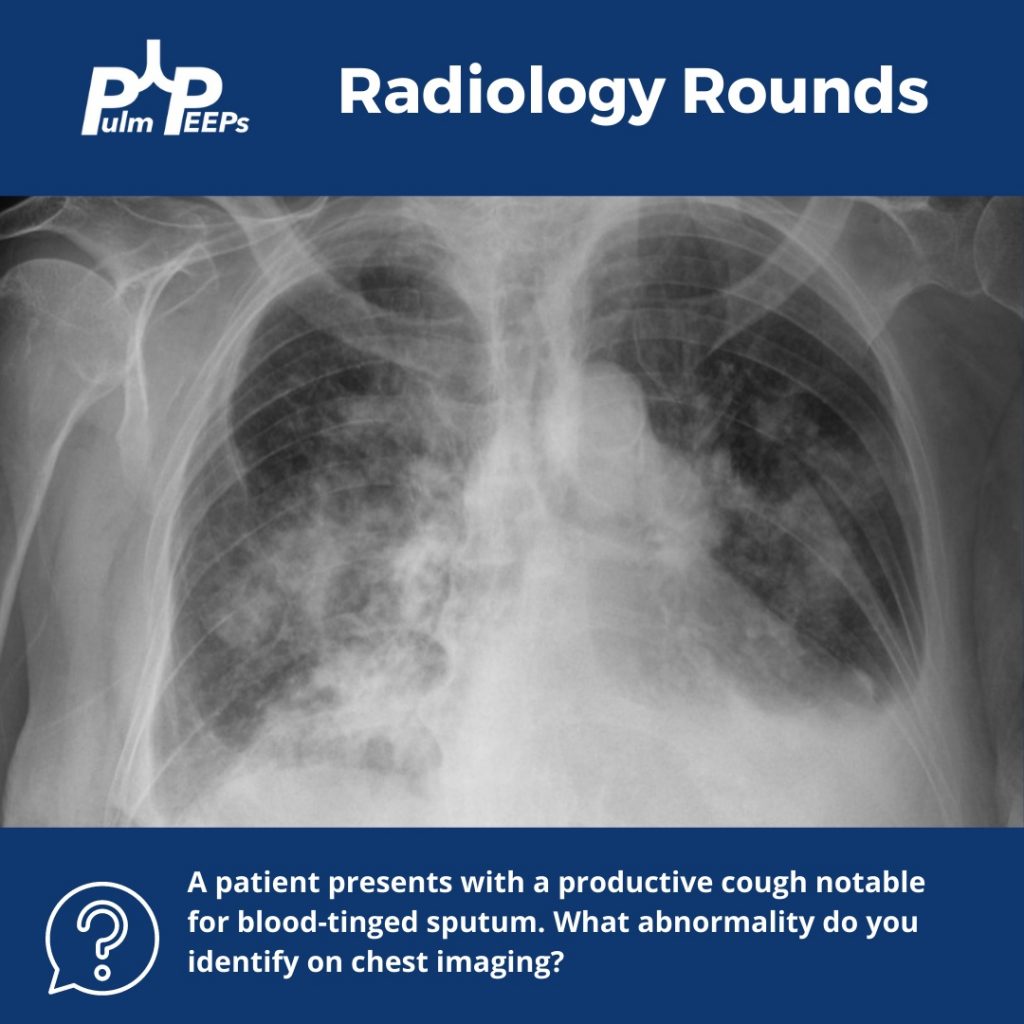
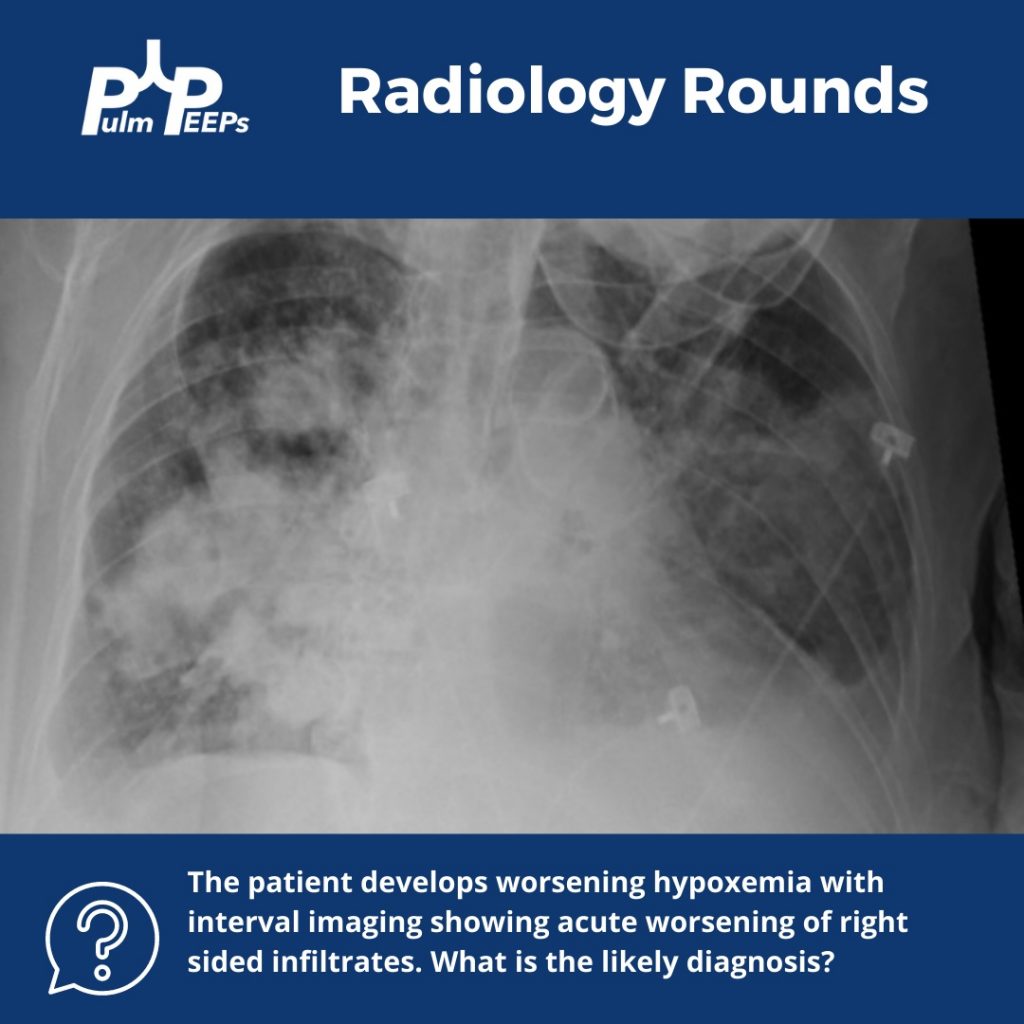
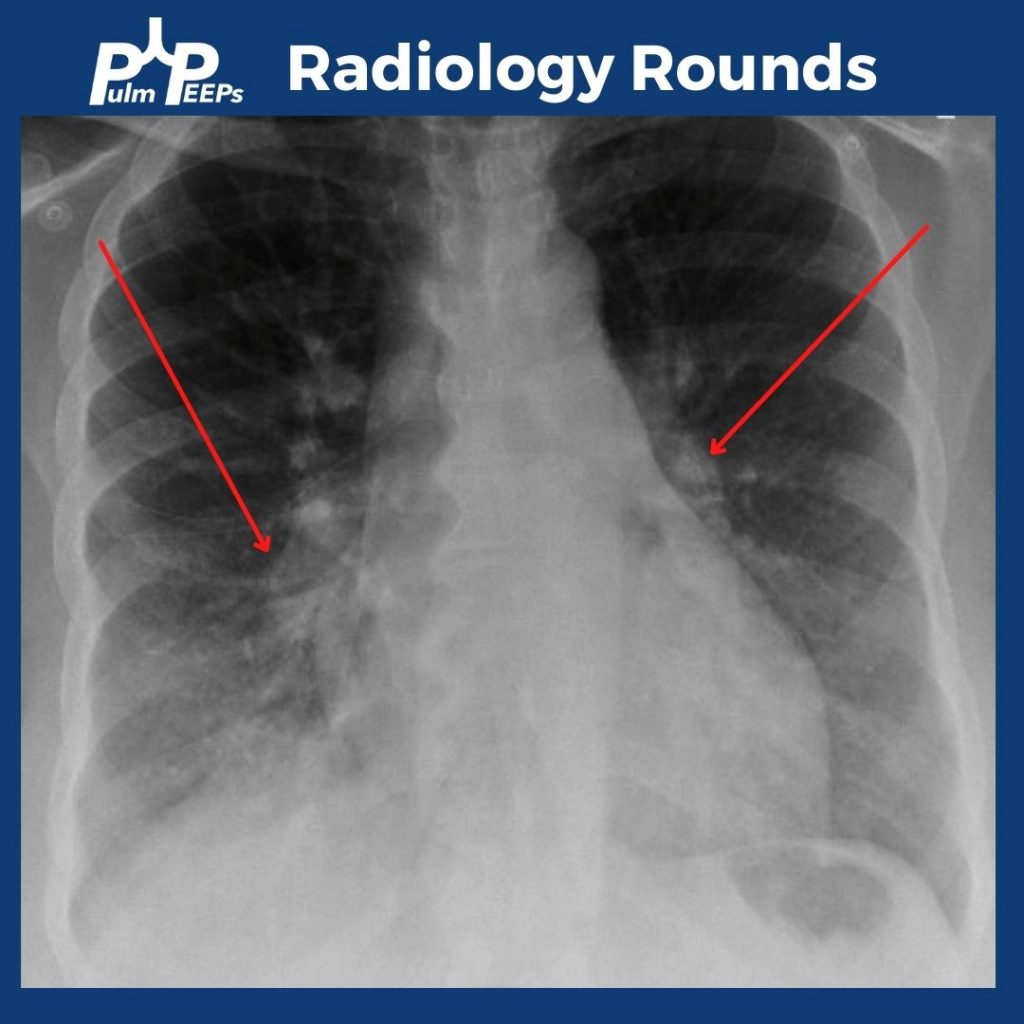
In addition to bibasilar opacities, the CXR shows bilateral enlarged pulmonary arteries.
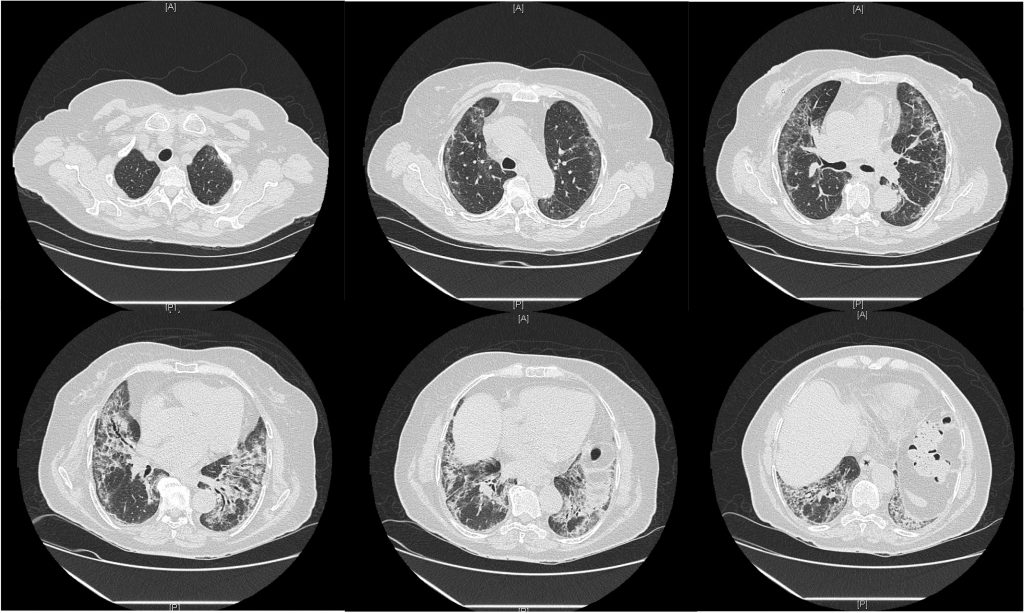
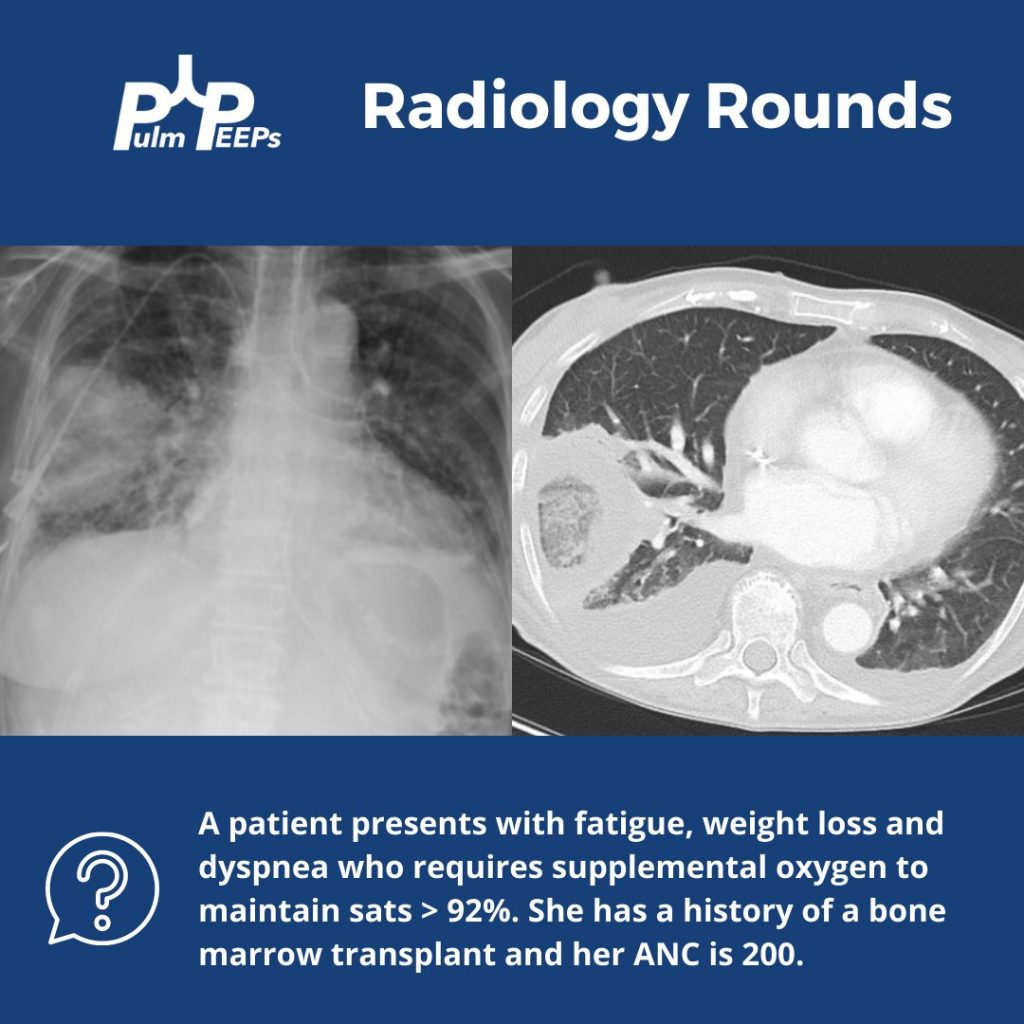
The patient was hypoxemic on room air and desatted into the 70s with ambulation. Given her possible connective tissue disease a CT chest was obtained.
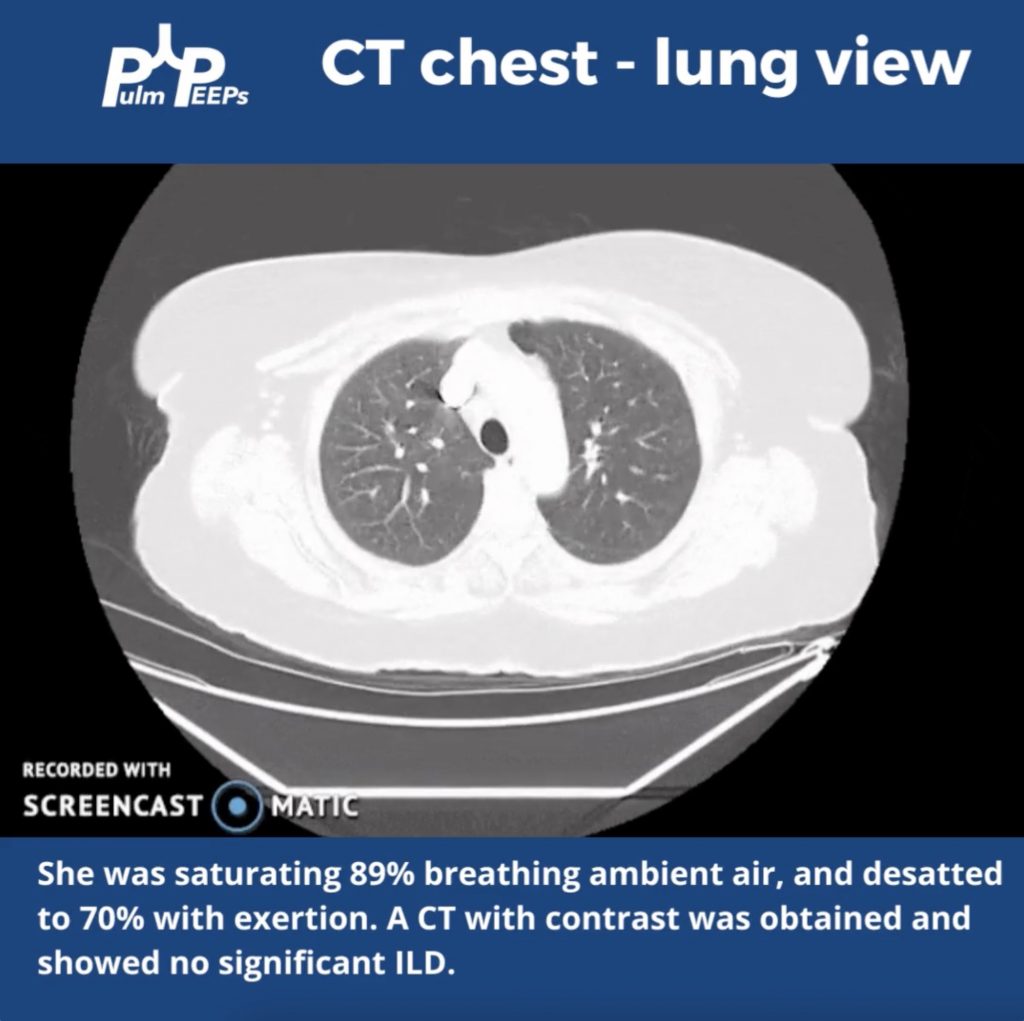
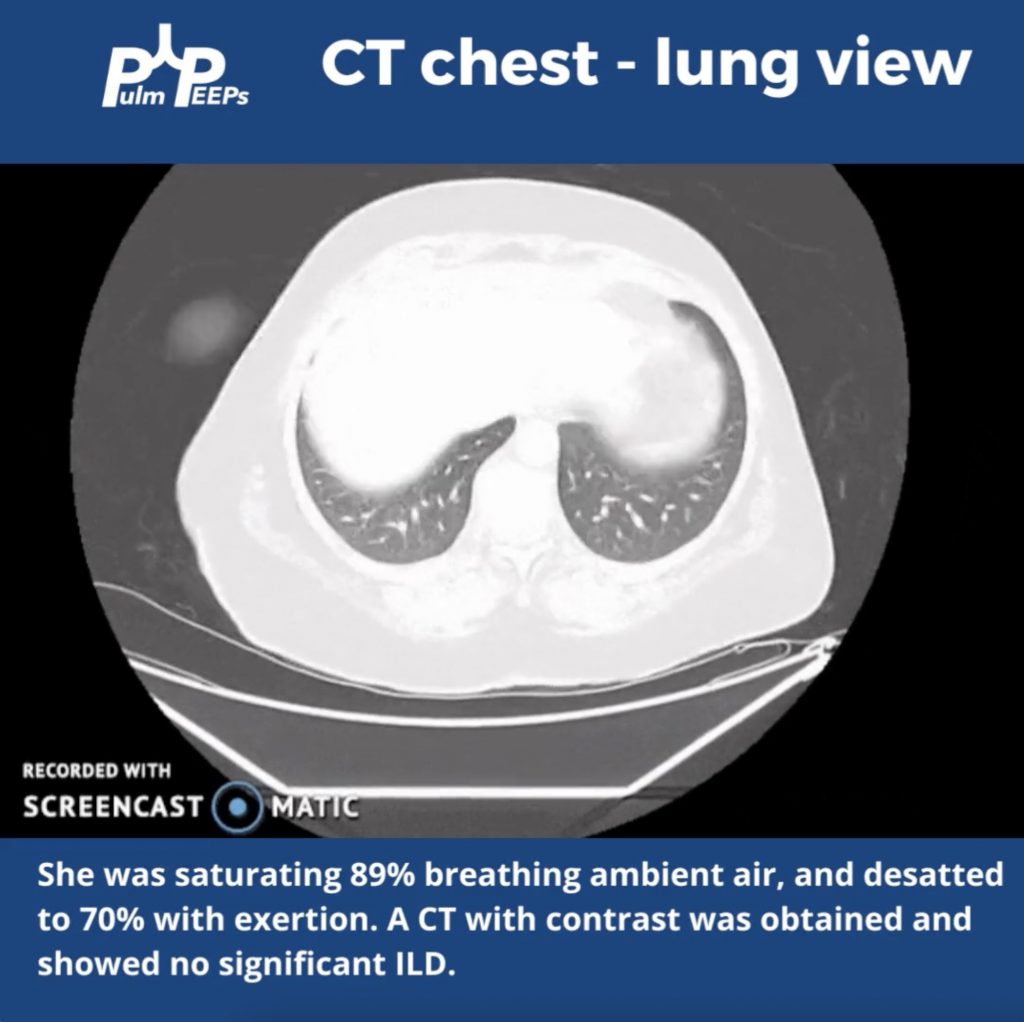
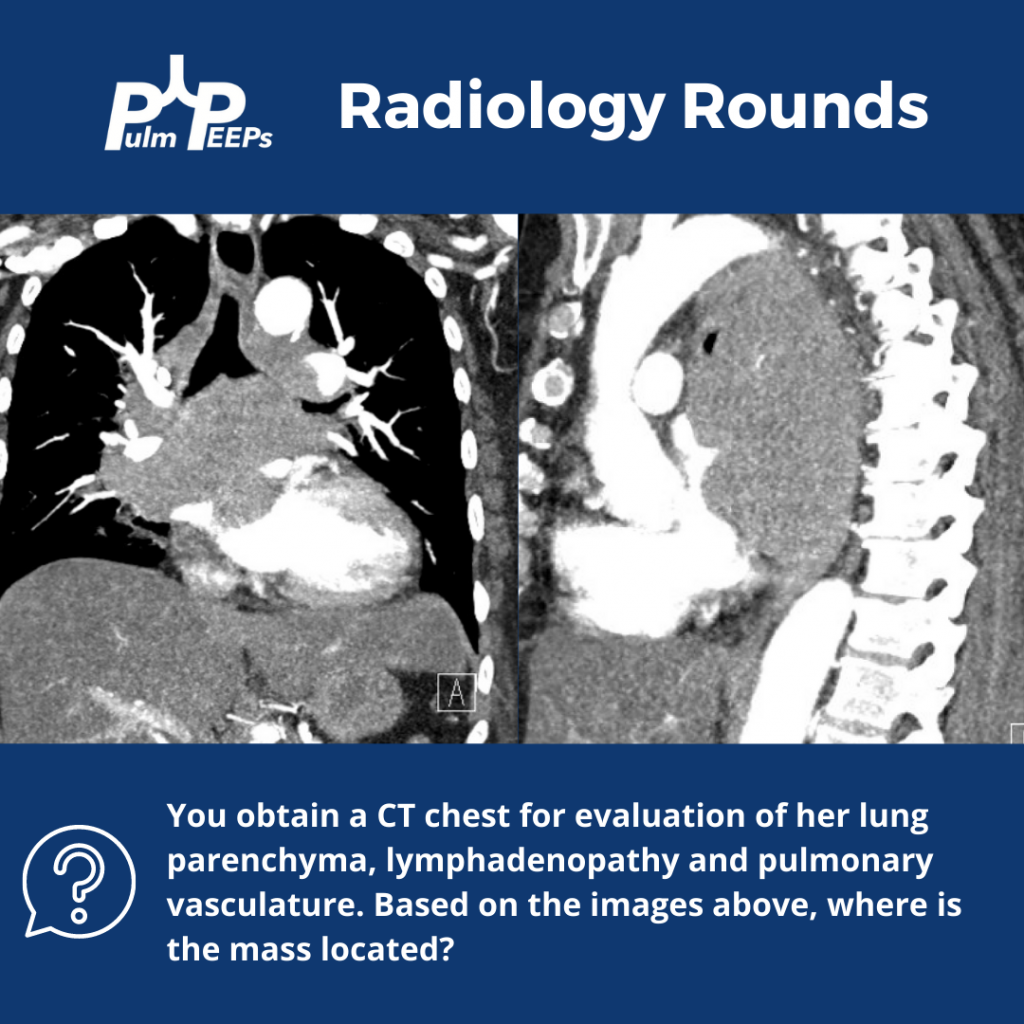
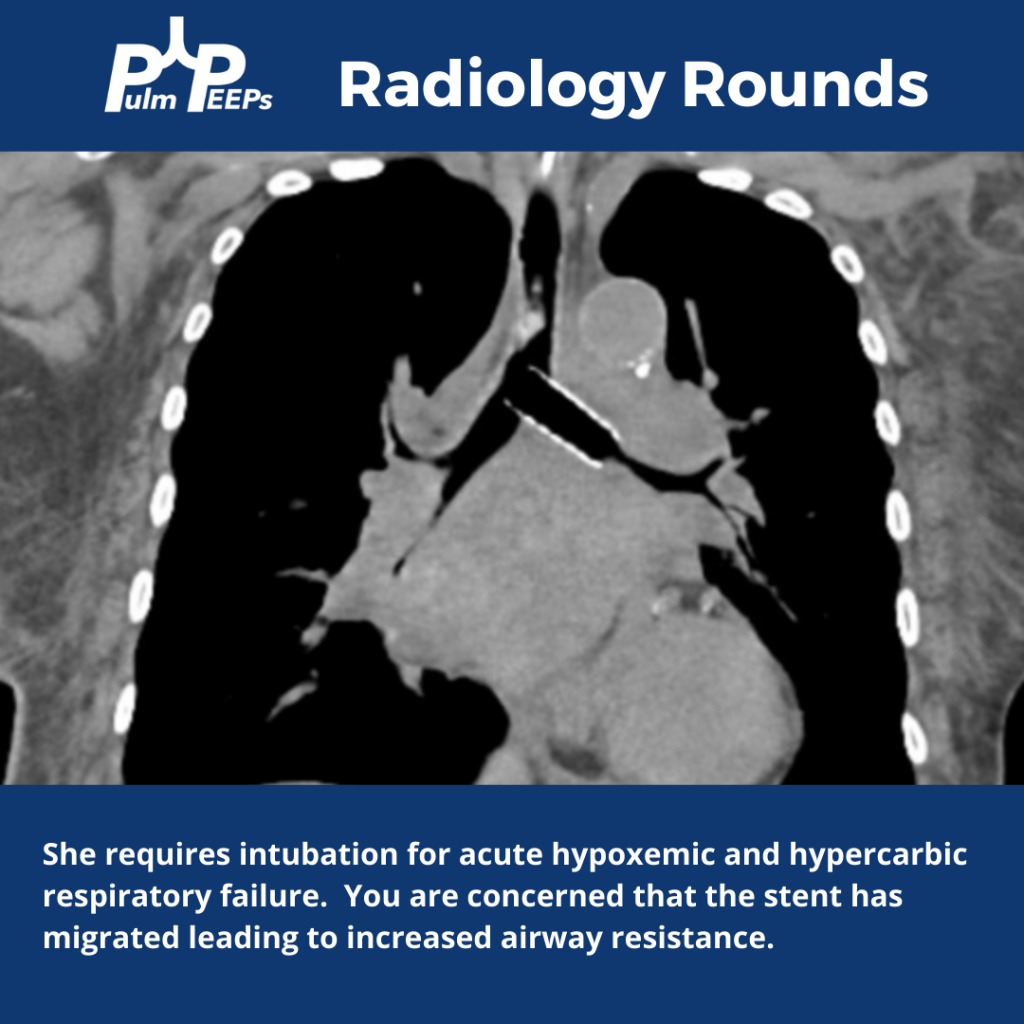
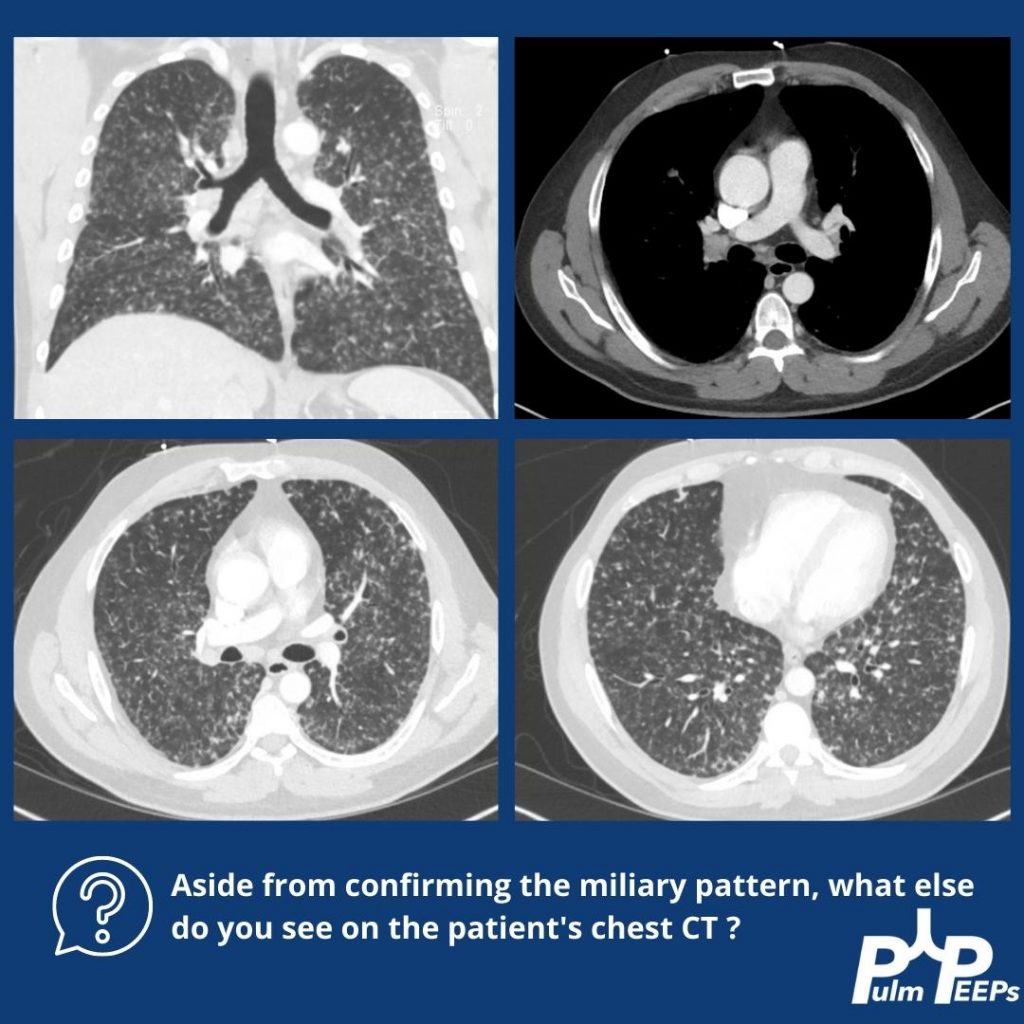
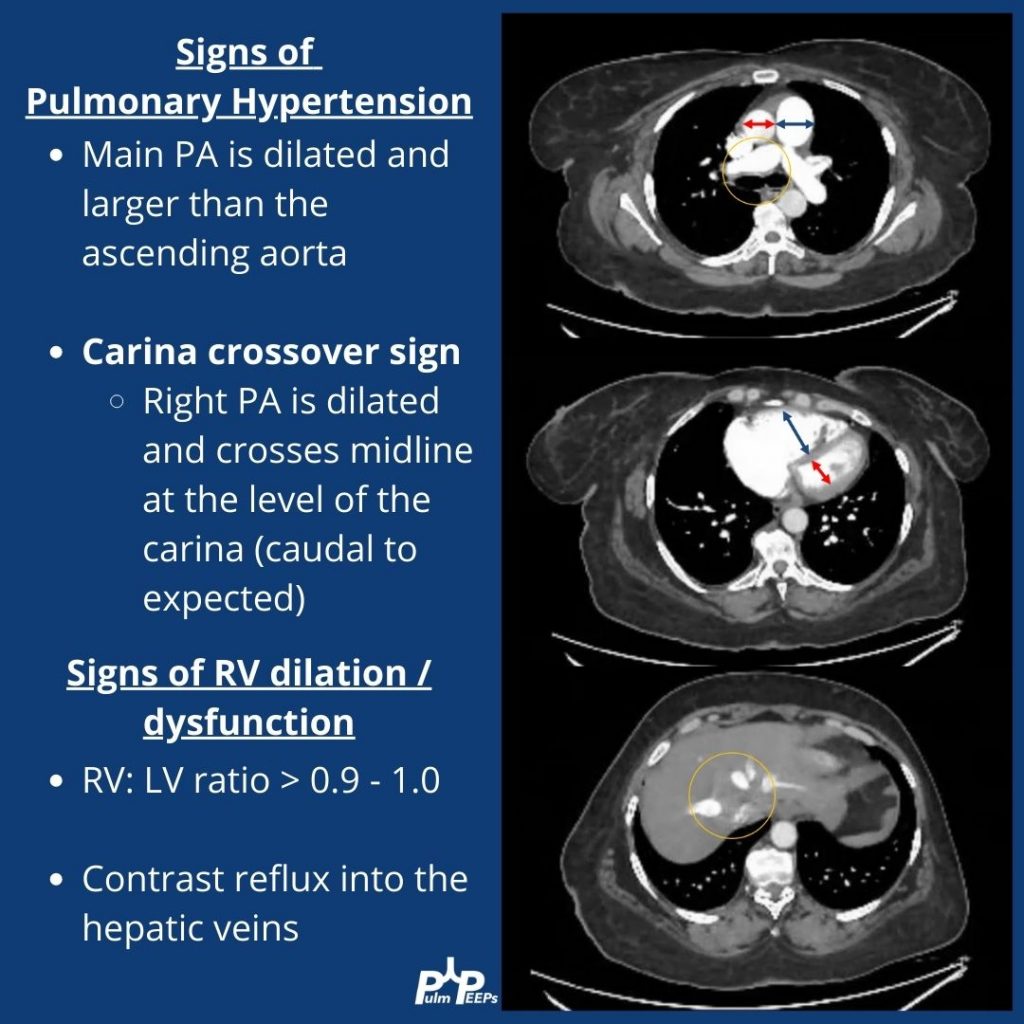
Although no ILD was revealed on the CT scan, let’s take a look at the mediastinal windows:
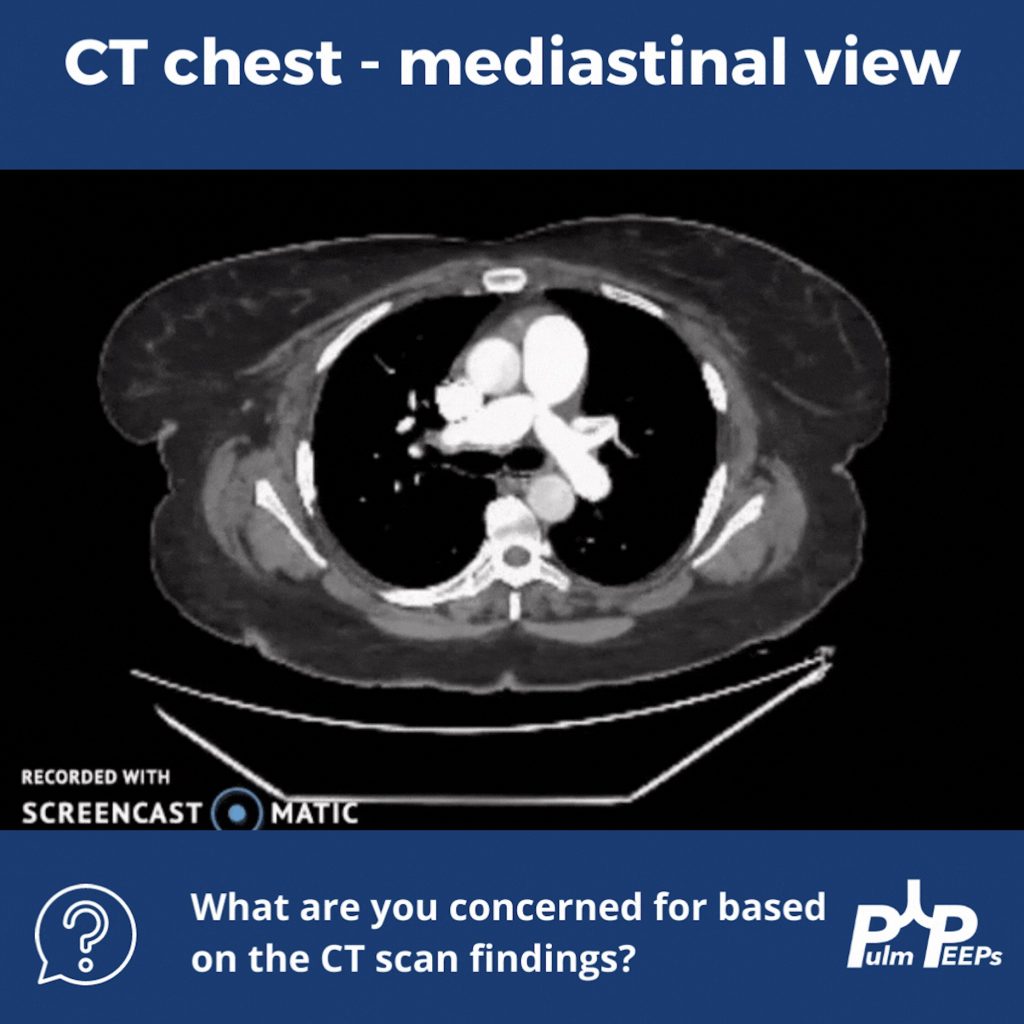
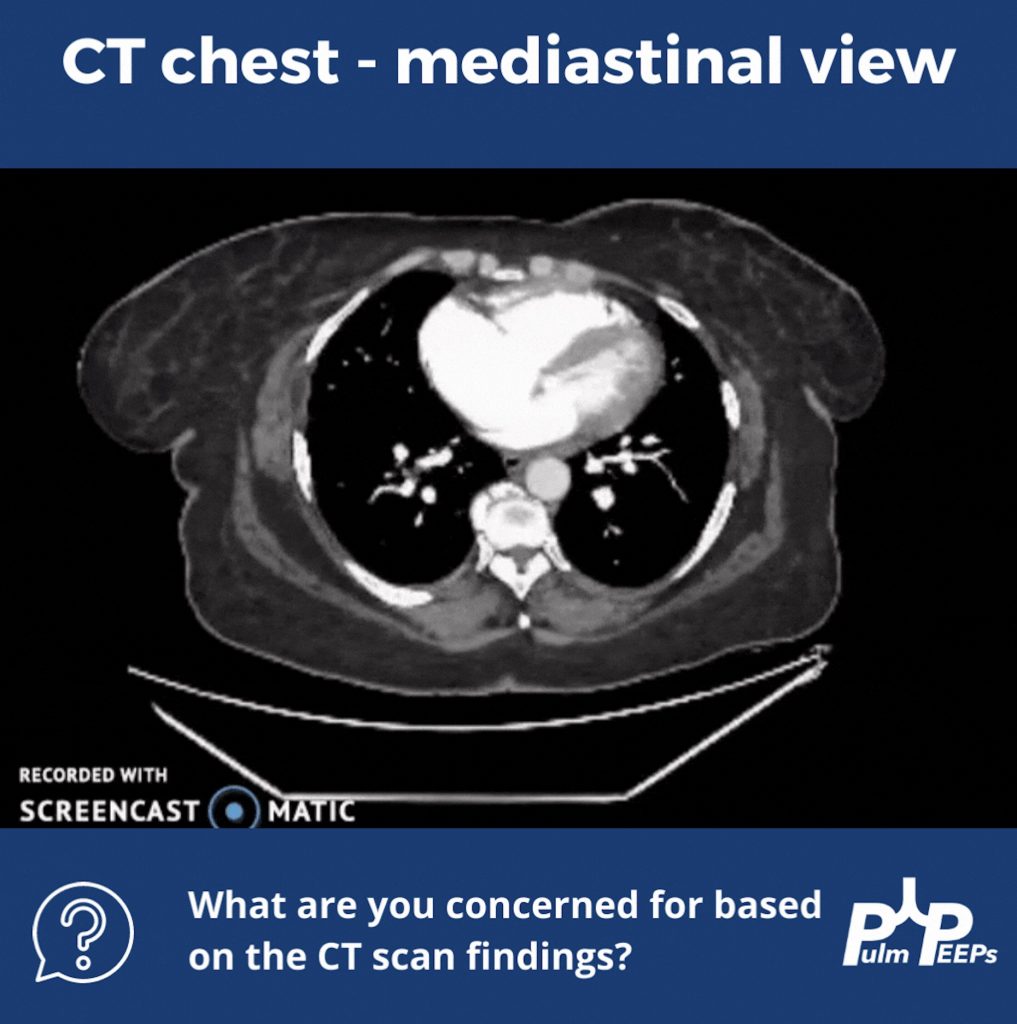
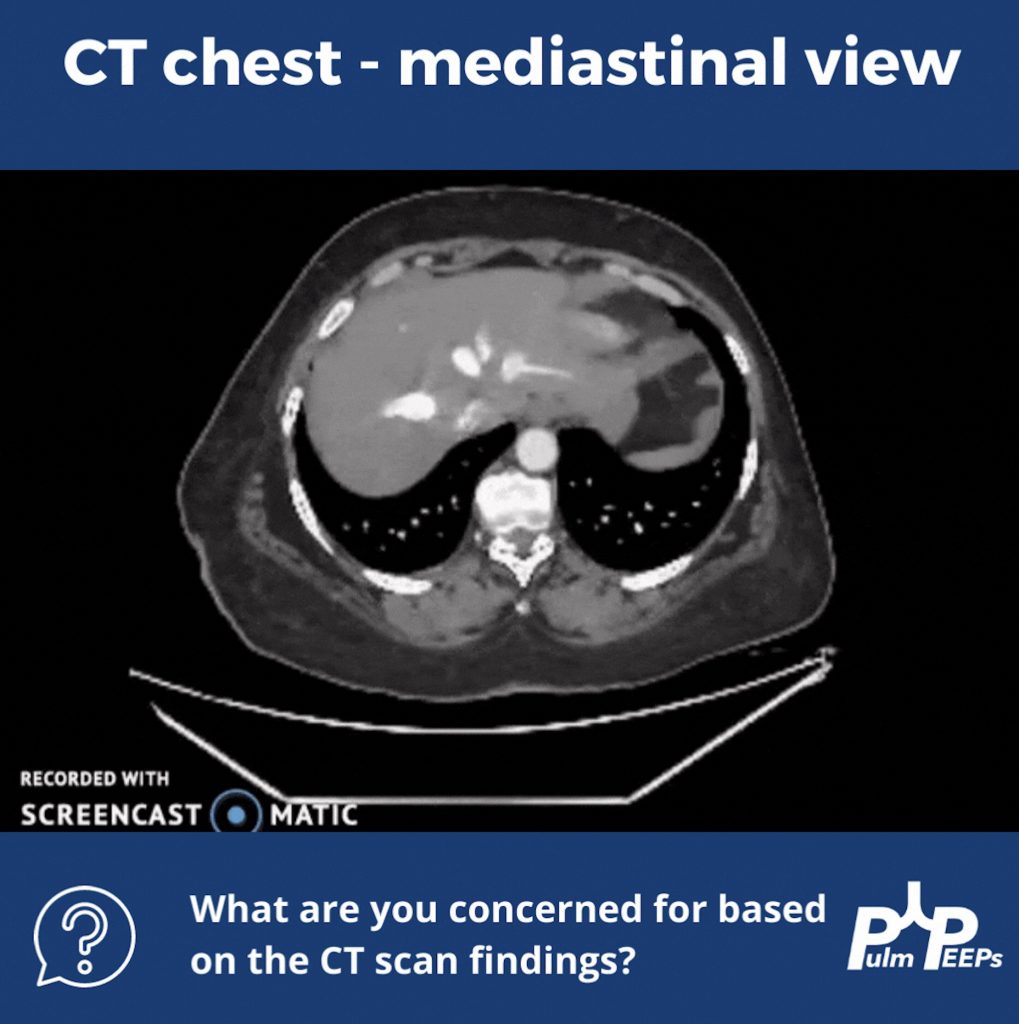
There are multiple signs of pulmonary hypertension, and right ventricular dilation and strain on this CT scan. Let’s review them:
To help explain the patient’s hypoxemia, an ECHO with bubble study was ordered next
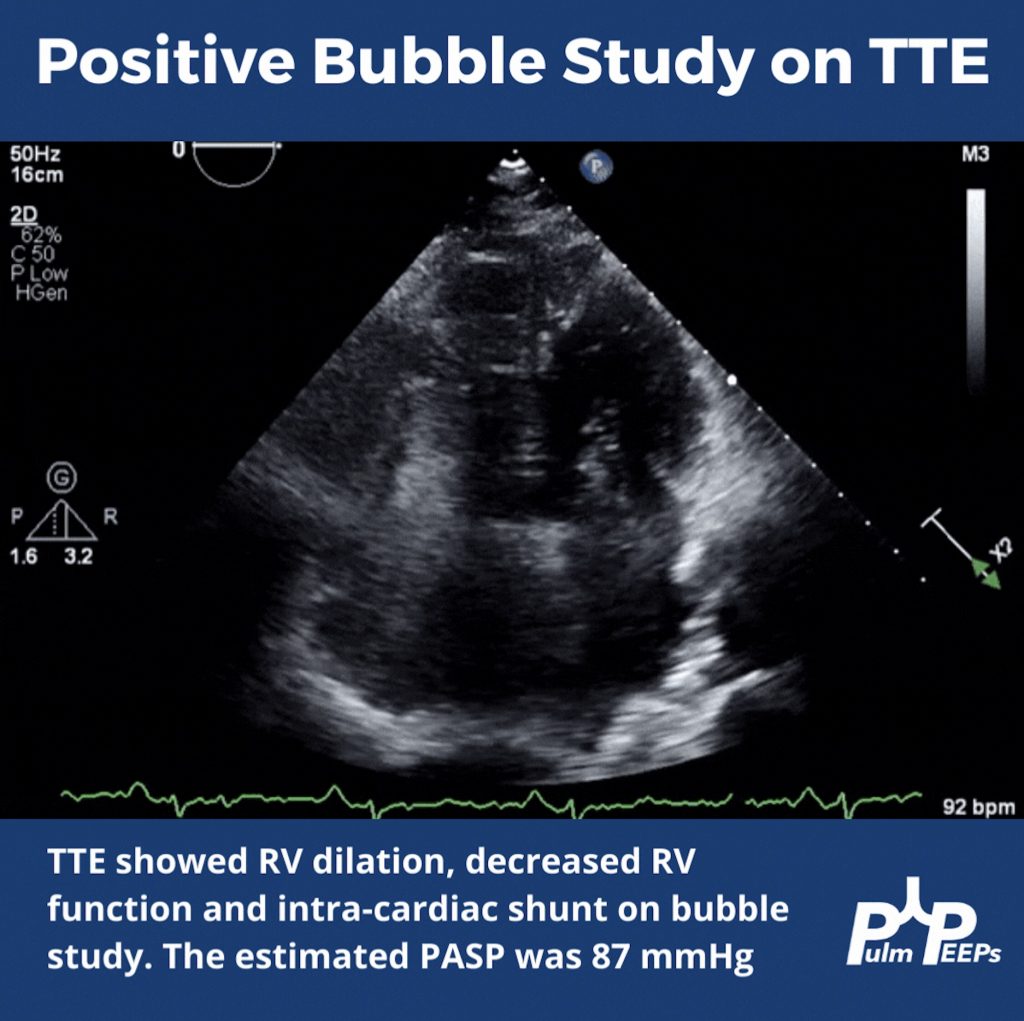
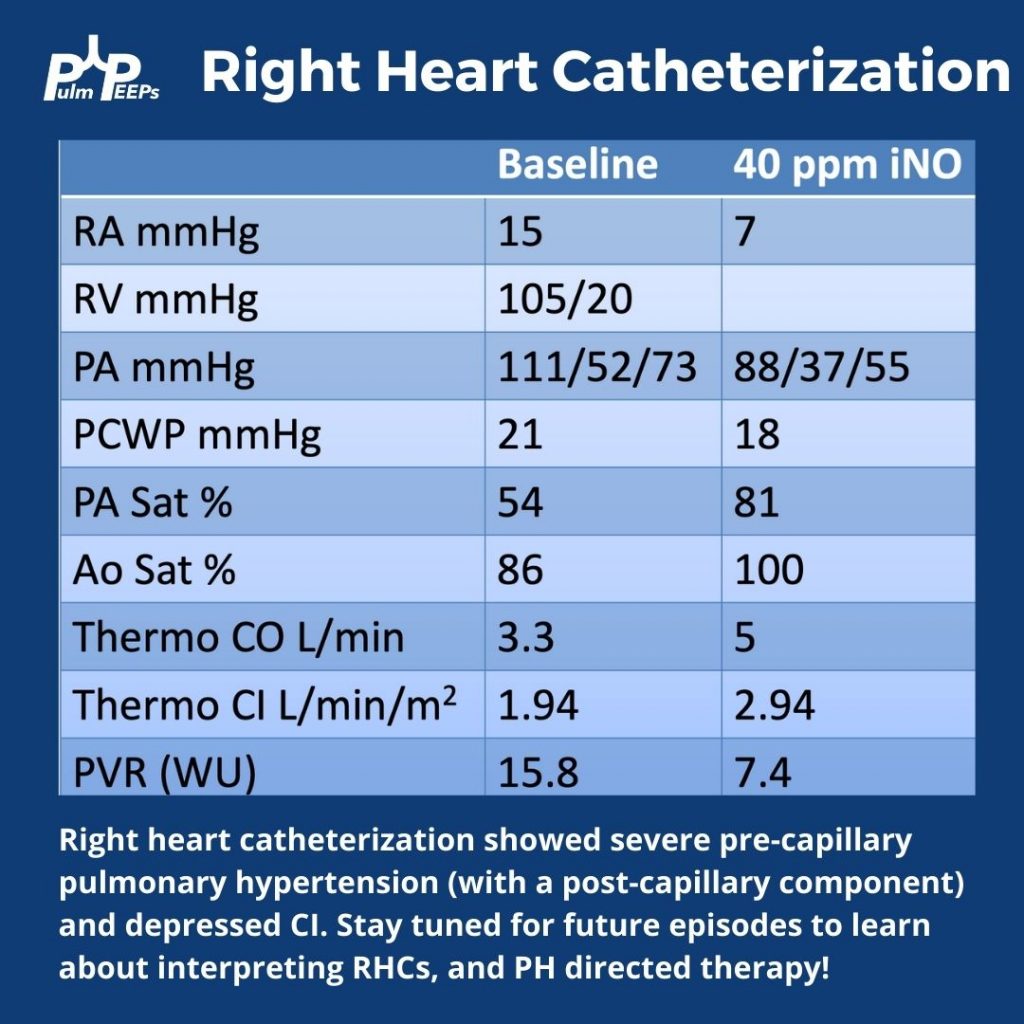
Since pulmonary hypertension can only truly be diagnosed on right heart catheterization, this was performed next and revealed severe pre- and post- (mostly pre)-capillary pulmonary hypertension