This week’s #RadiologyRounds is authored by Leon Mirson, one of our amazing Associate Editors. Follow us on Twitter to answer live polls about the case and future Radiology Rounds cases!

This week’s #RadiologyRounds is authored by Leon Mirson, one of our amazing Associate Editors. Follow us on Twitter to answer live polls about the case and future Radiology Rounds cases!
Time for another #RadiologyRounds! This case is authored by PulmPEEPs associate editor @TessLitchman. Great teaching ahead!
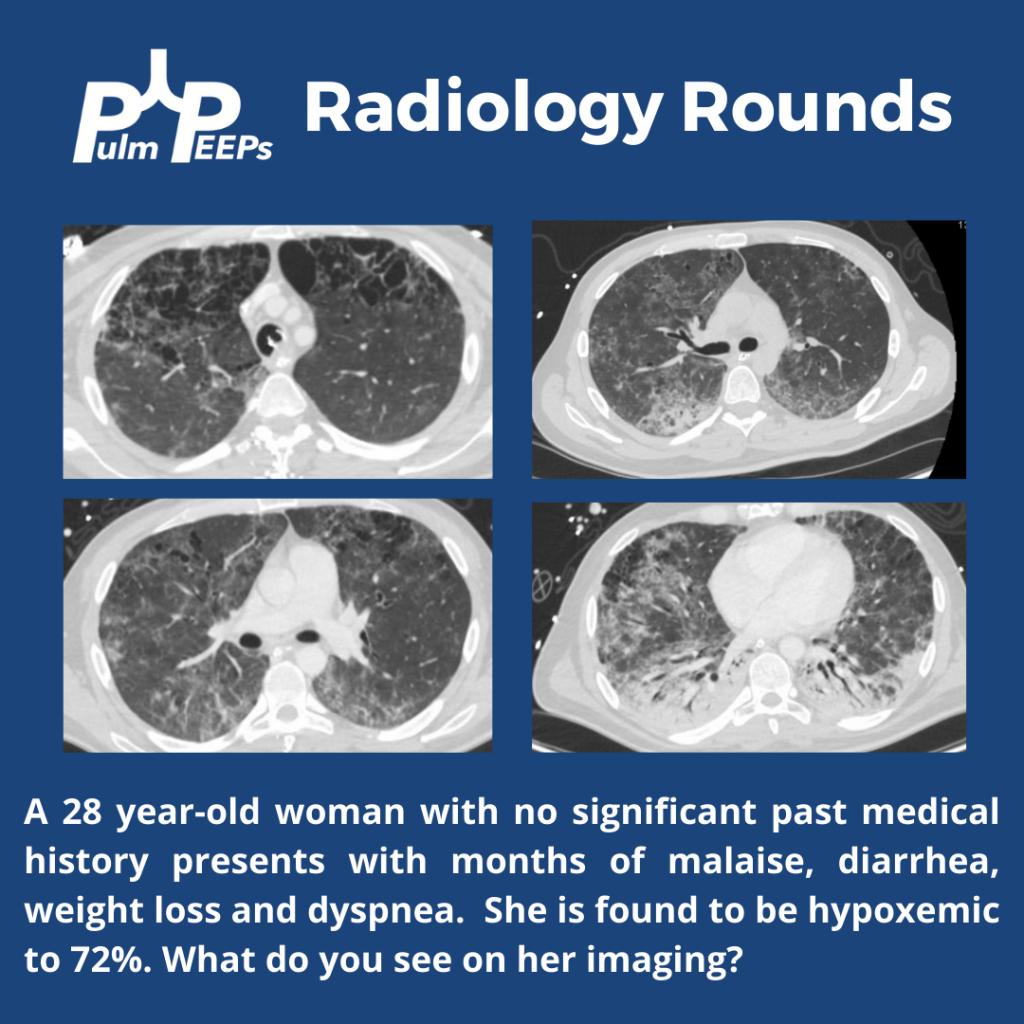
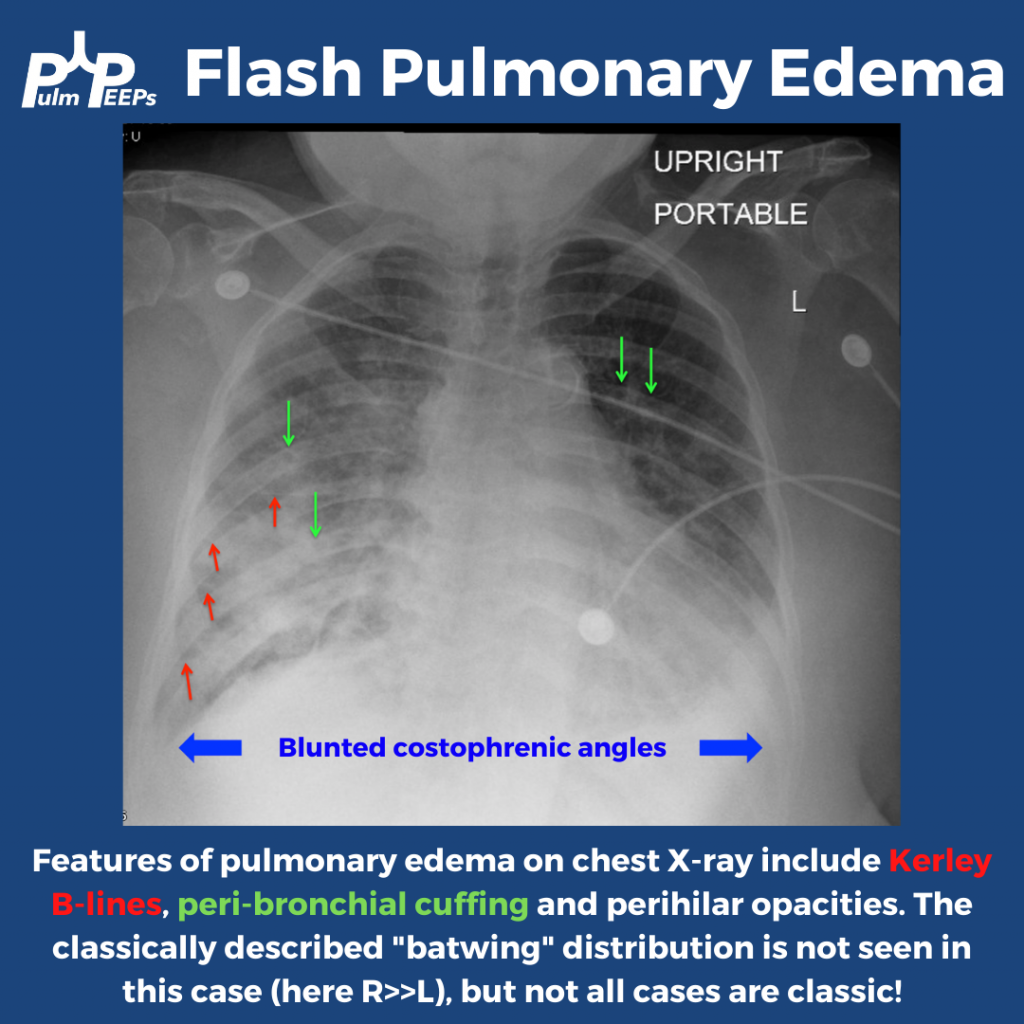
Trick question (sorry)! All of these features are present.
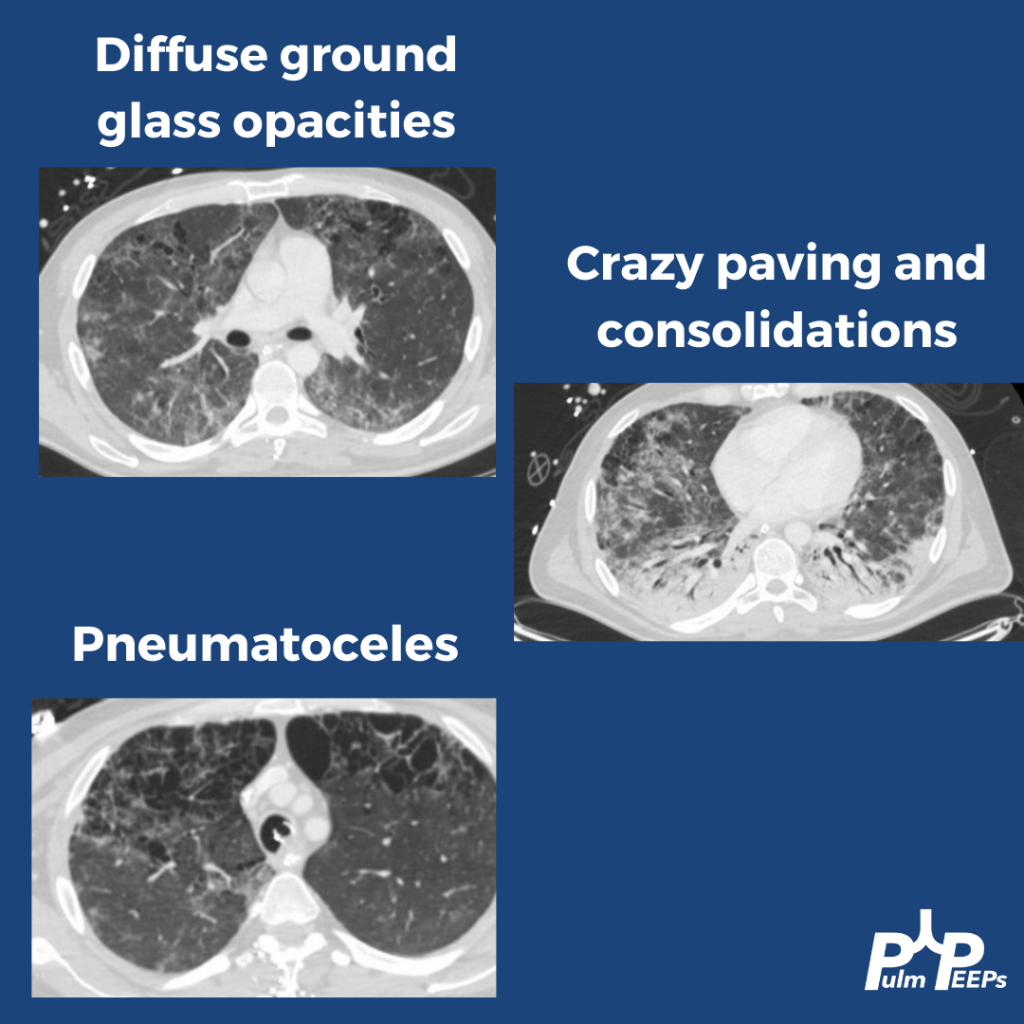
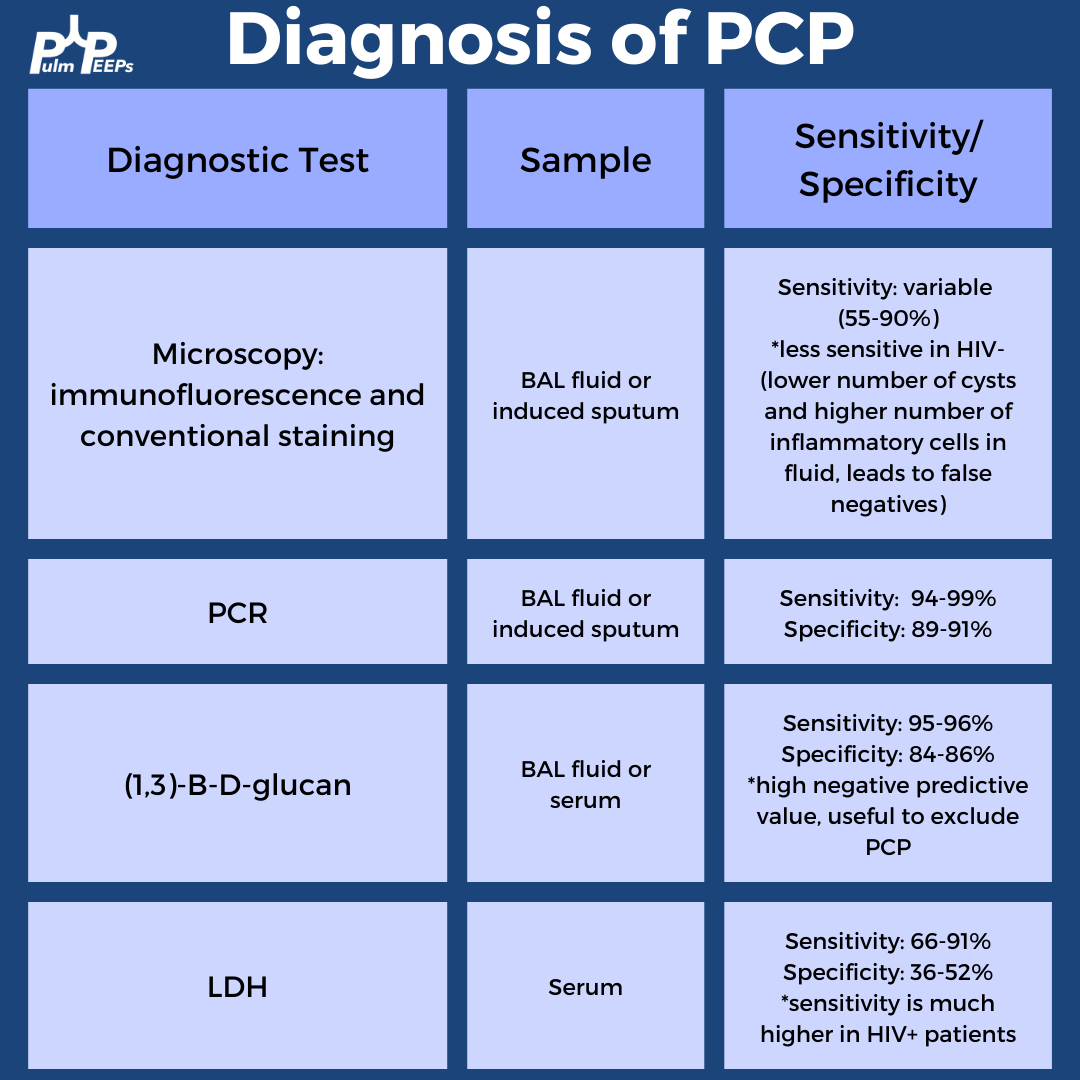
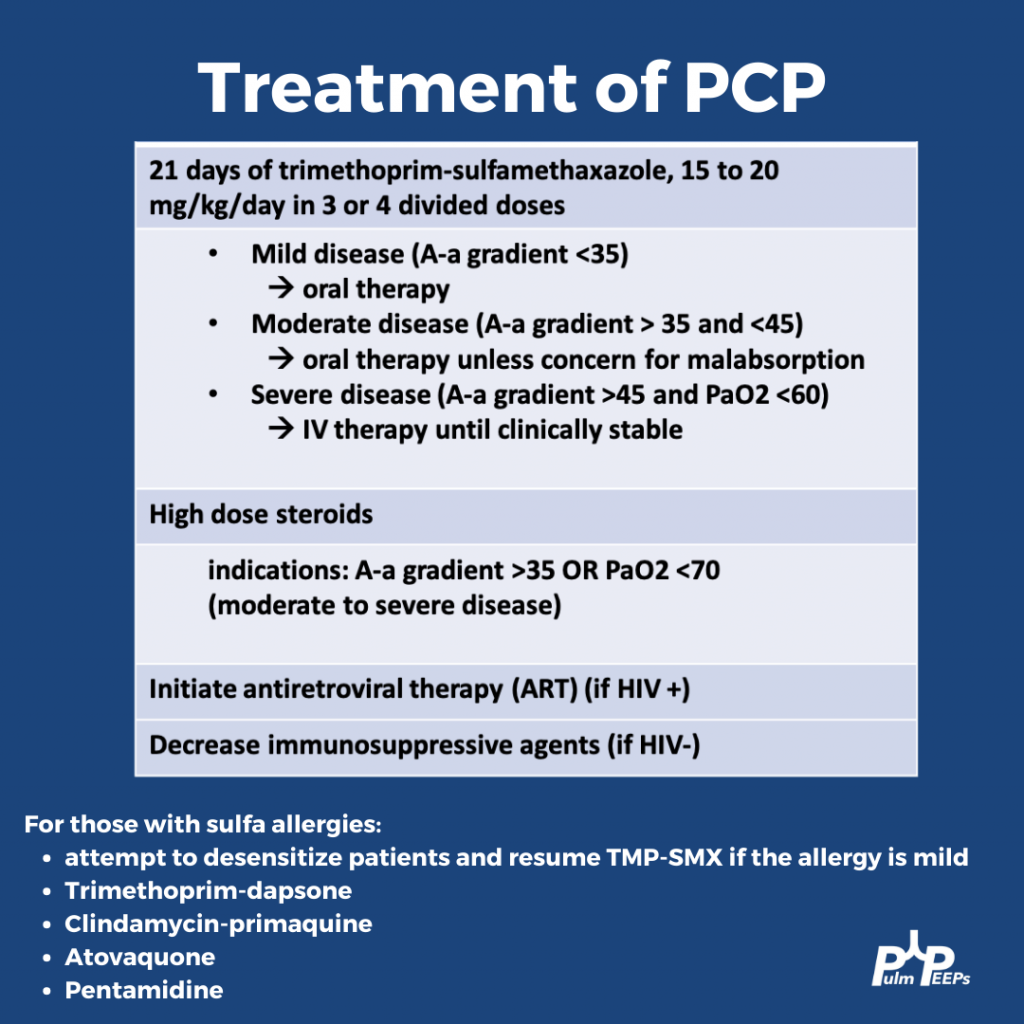
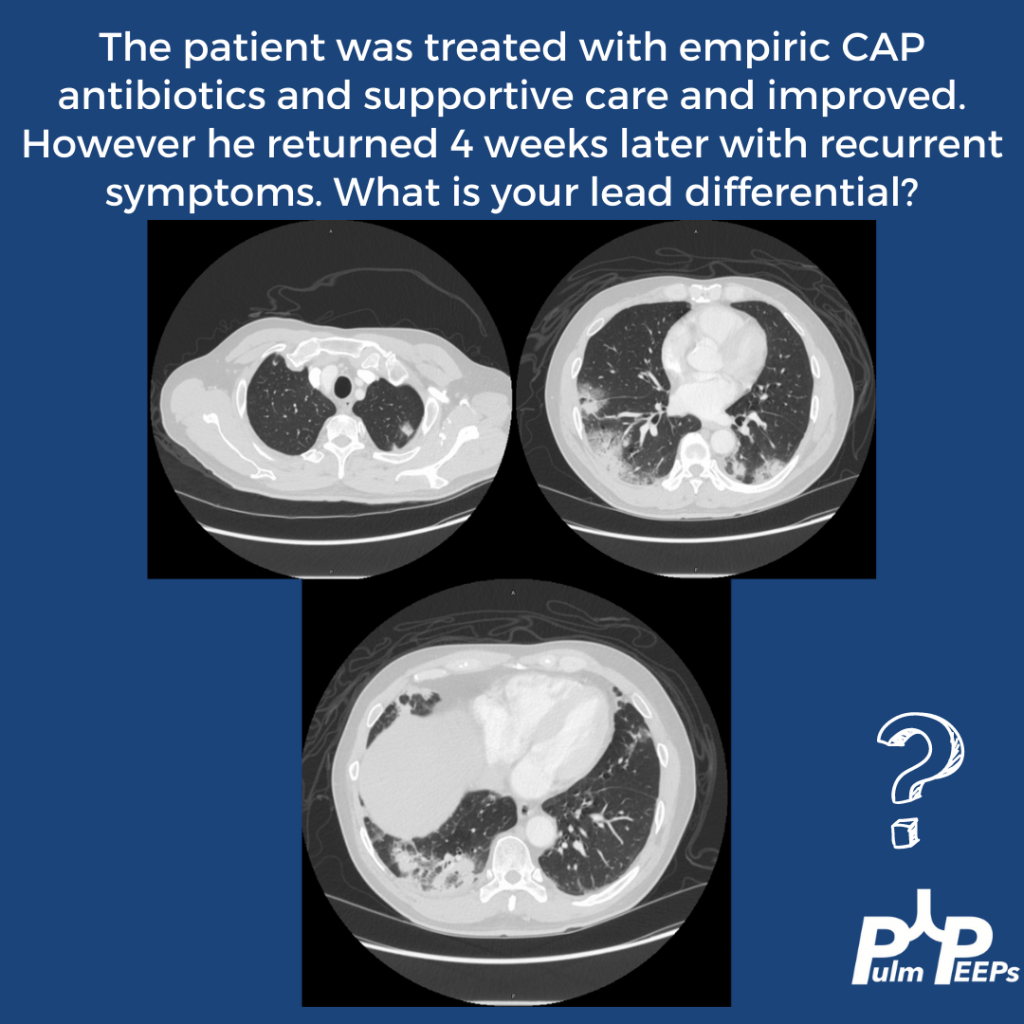
A bronchoscopy was performed and the patient was diagnosed with PCP. Additional testing confirmed a new diagnosis of HIV.
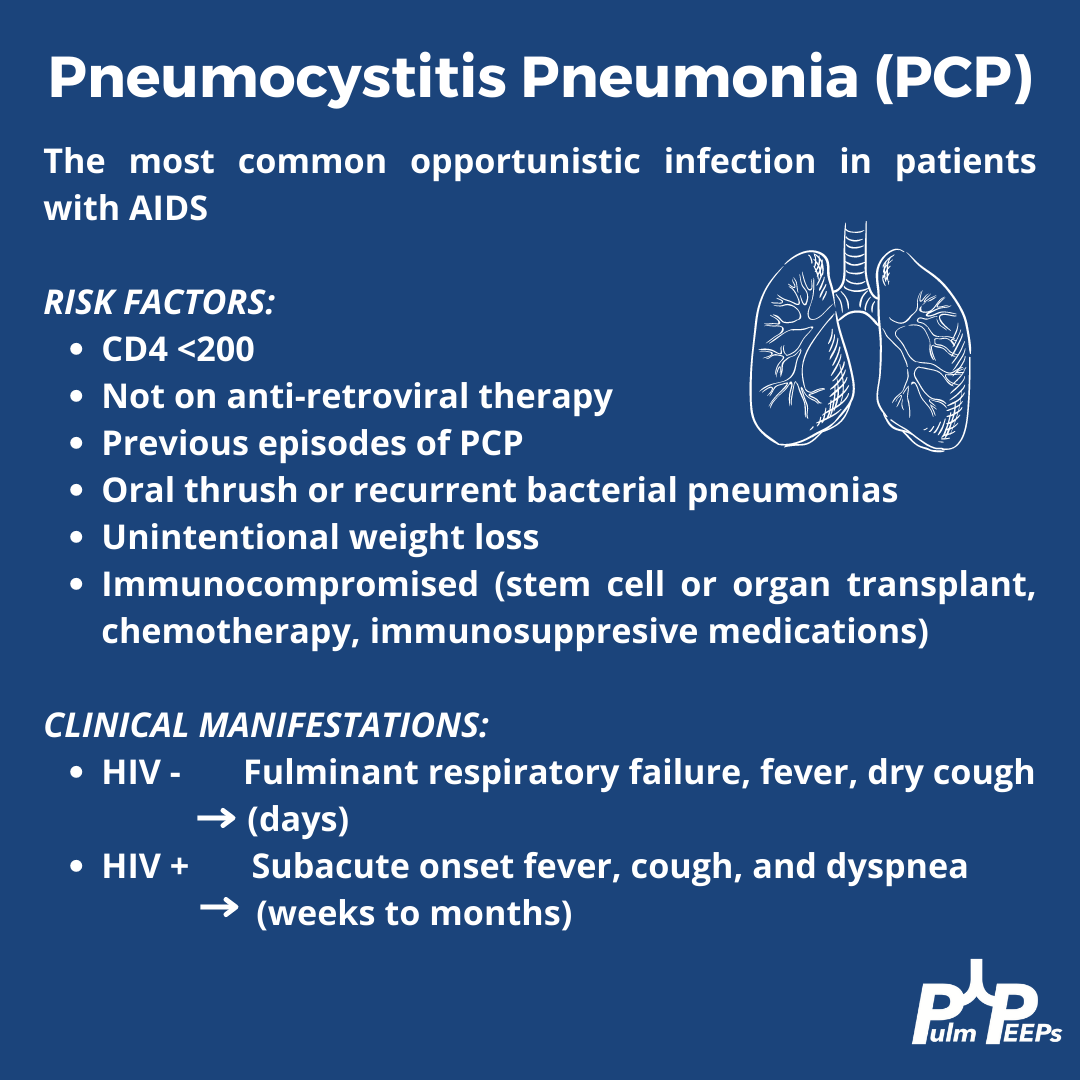
This patient was treated with high-dose Bactrim and IV steroids, in addition to being started on ART.
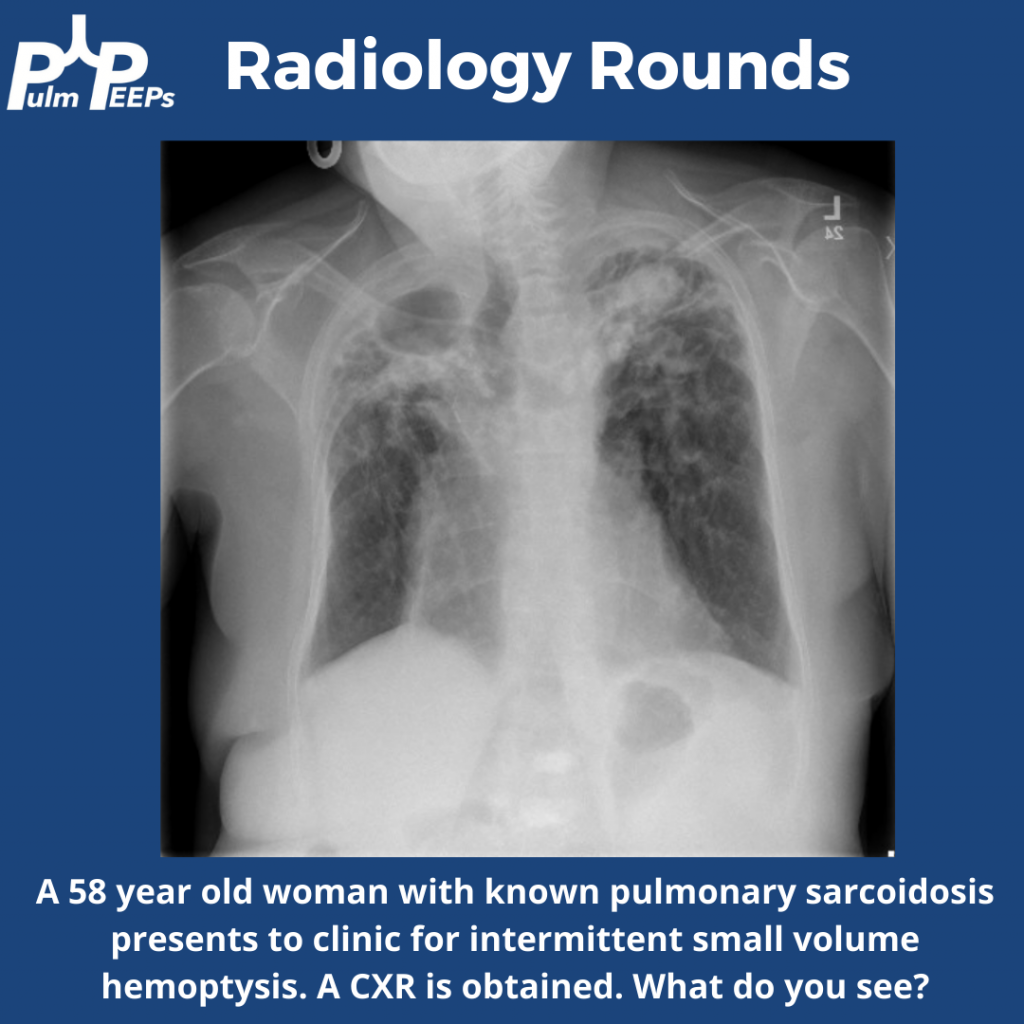
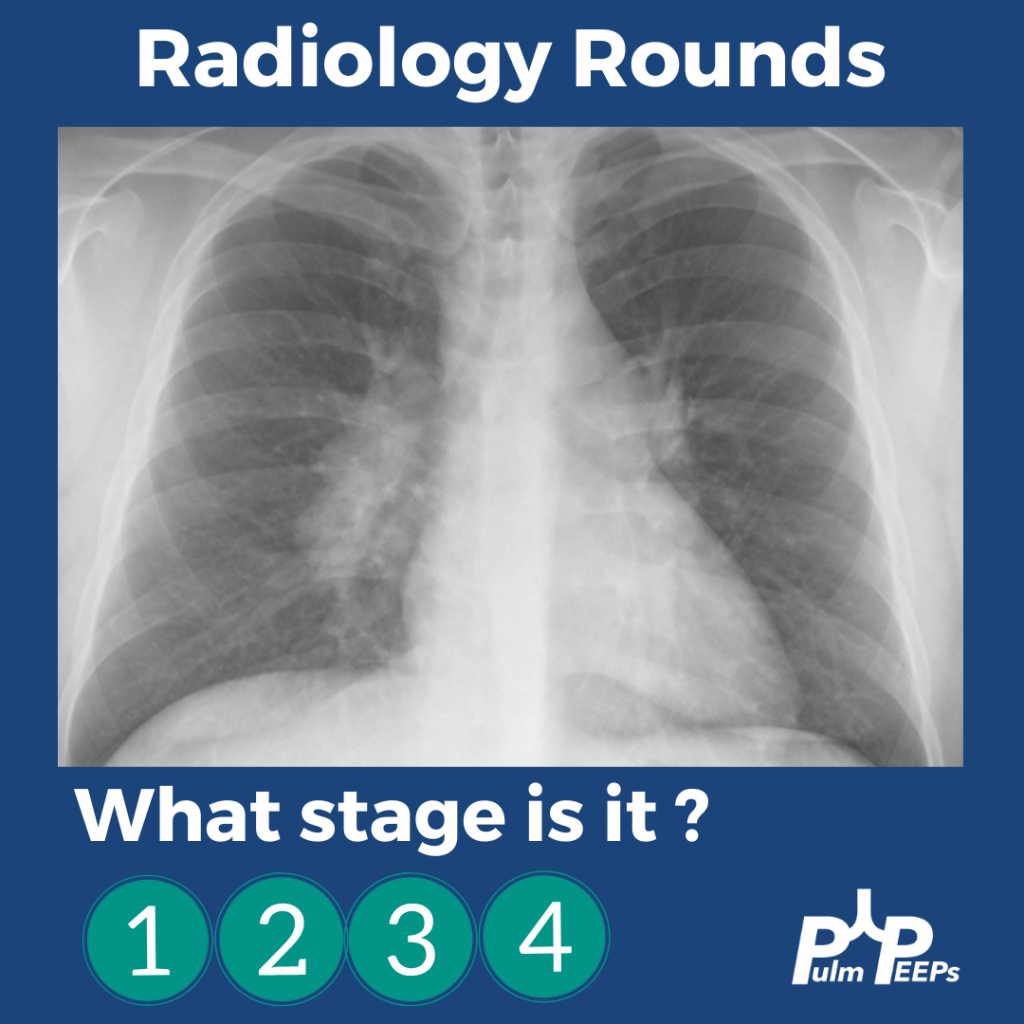
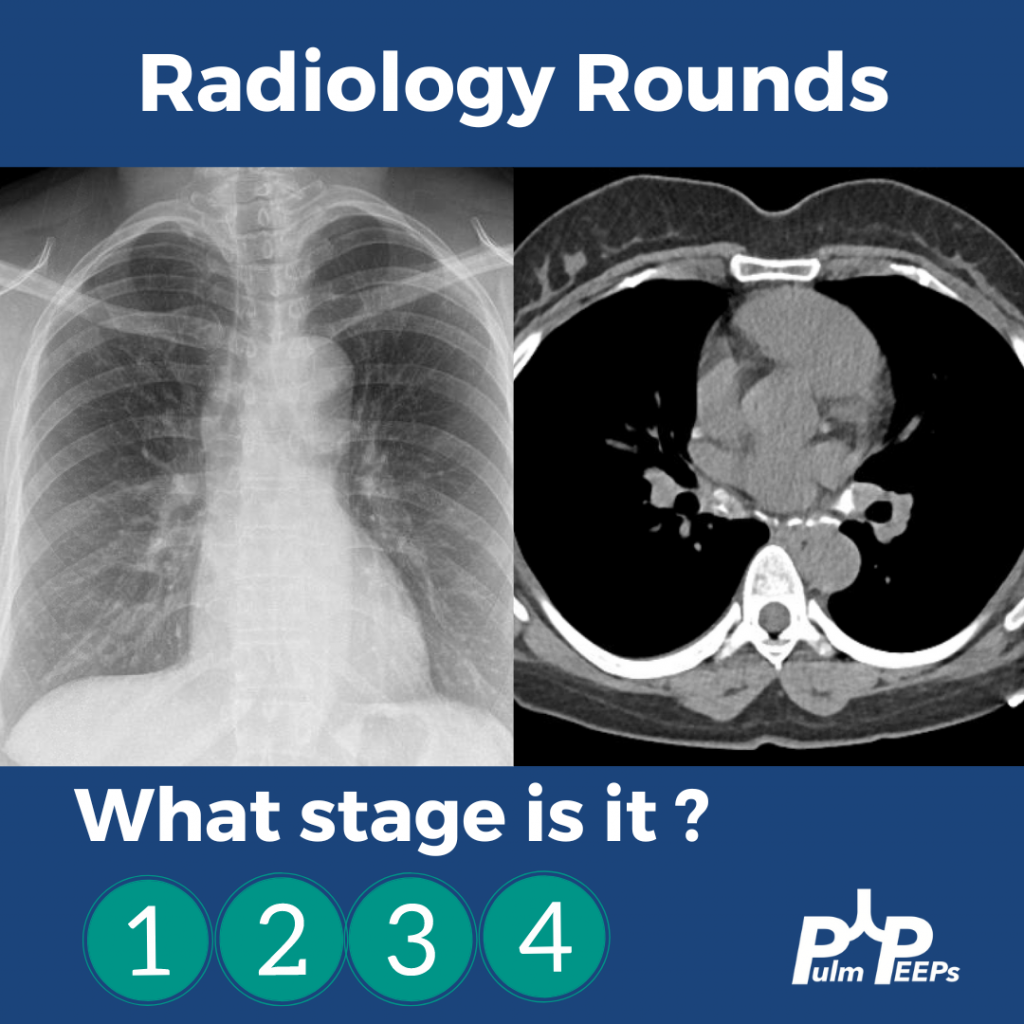
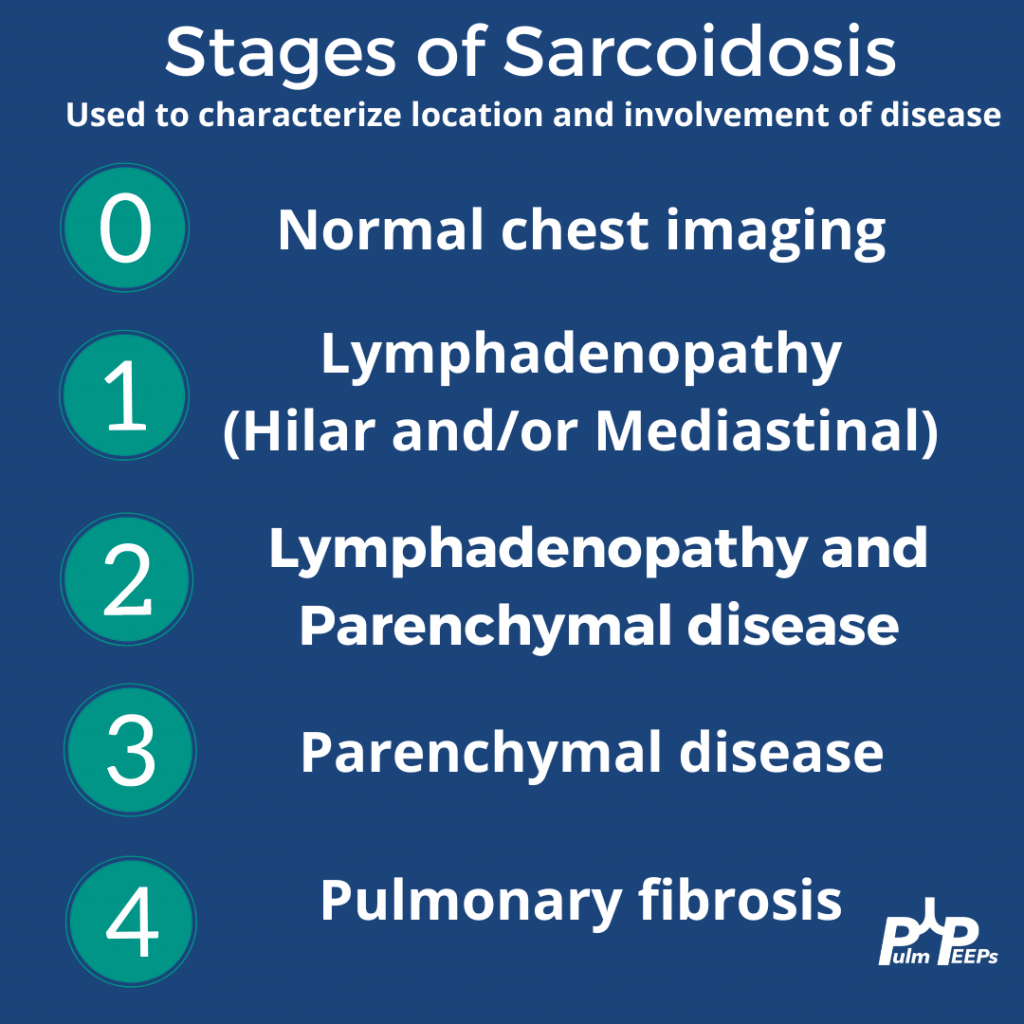
It is Tuesday and we have another Radiology Rounds we can’t wait to share with you. Follow along and see if you select the right answer as we go through different presentations of sarcoidosis and pick your answer! What stage is it?!
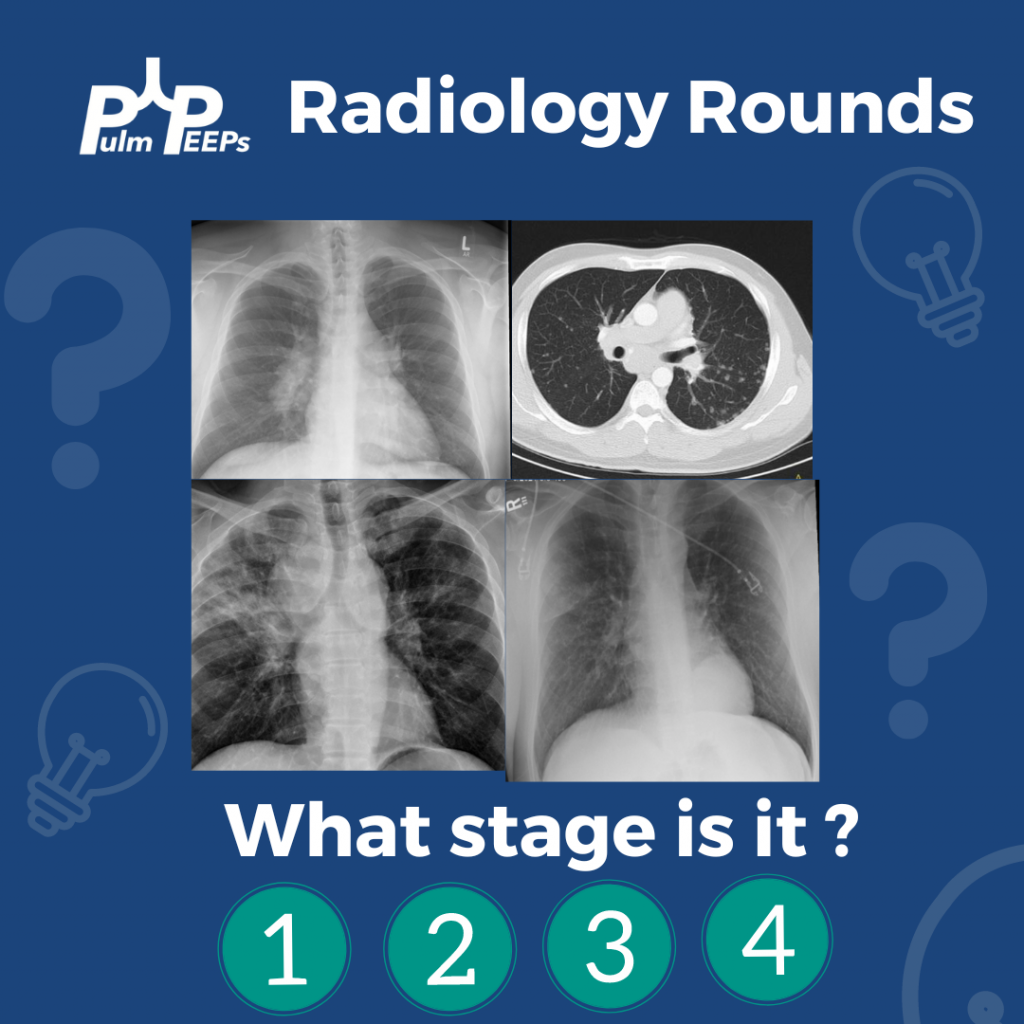
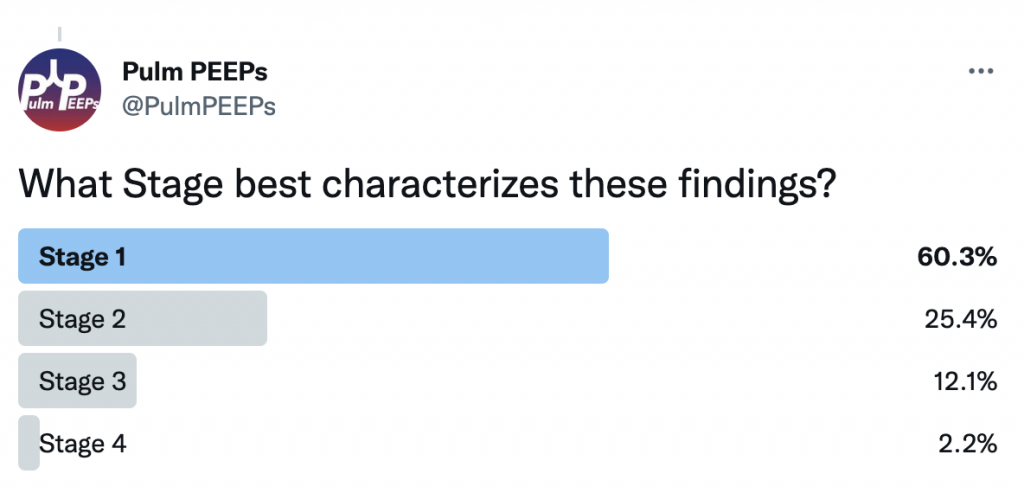
A middle-aged man presents to you after he was found to have hilar adenopathy on a routine chest x-ray.
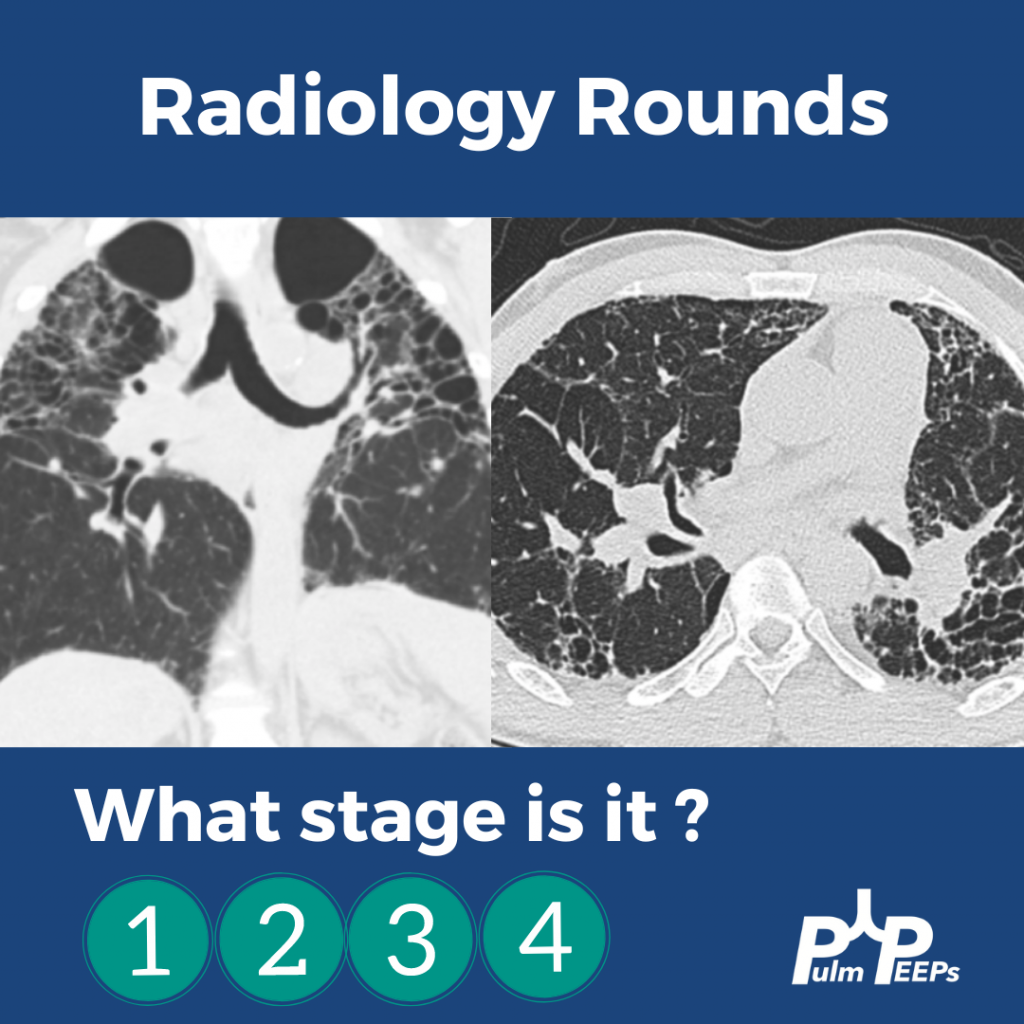
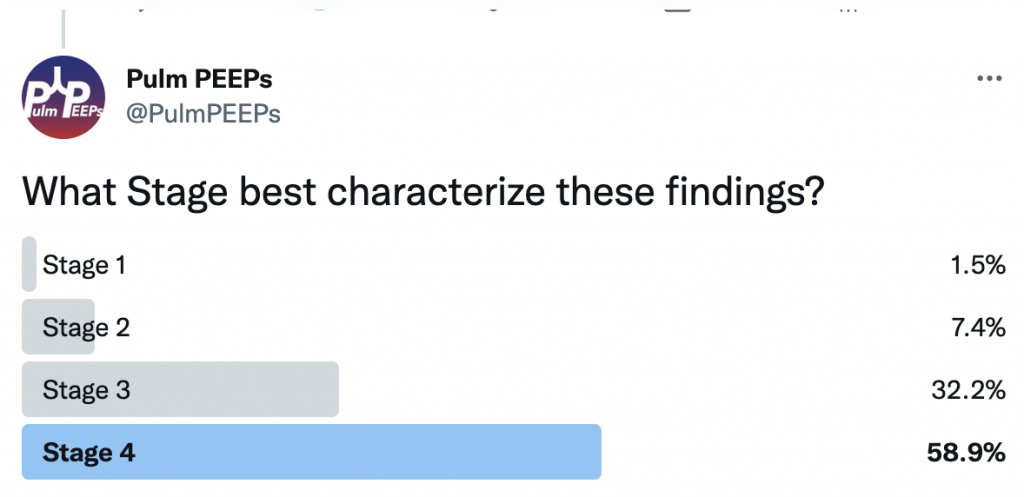
A middle-age man presents with dyspnea on exertion, night sweats and weight loss. You see evidence of bilateral apical disease, and fibrosis with evidence of honeycombing on chest CT.
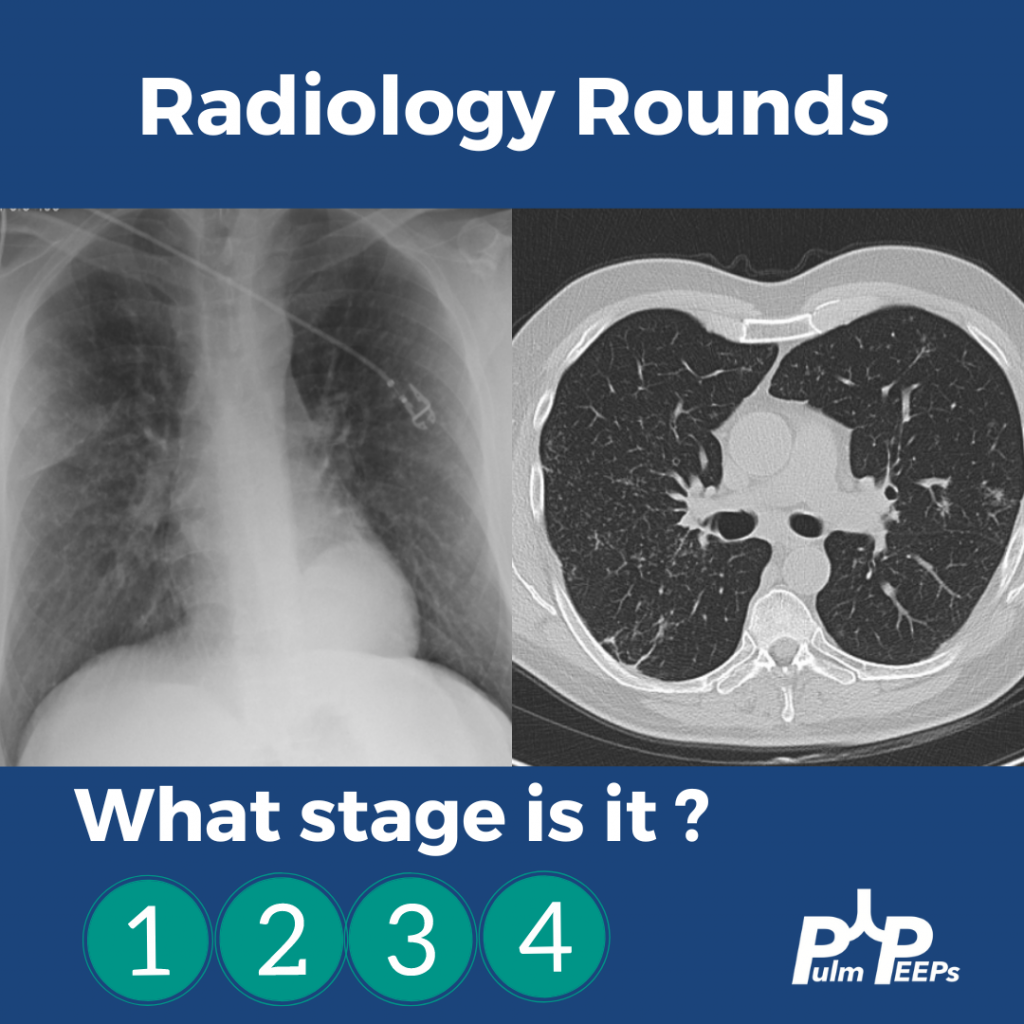
A young woman presents with dyspnea on exertion and was found to have hilar adenopathy with parenchymal disease.
An elderly man presents with dyspnea on exertion and was found to have nodular parenchymal disease without extensive lymphadenopathy.
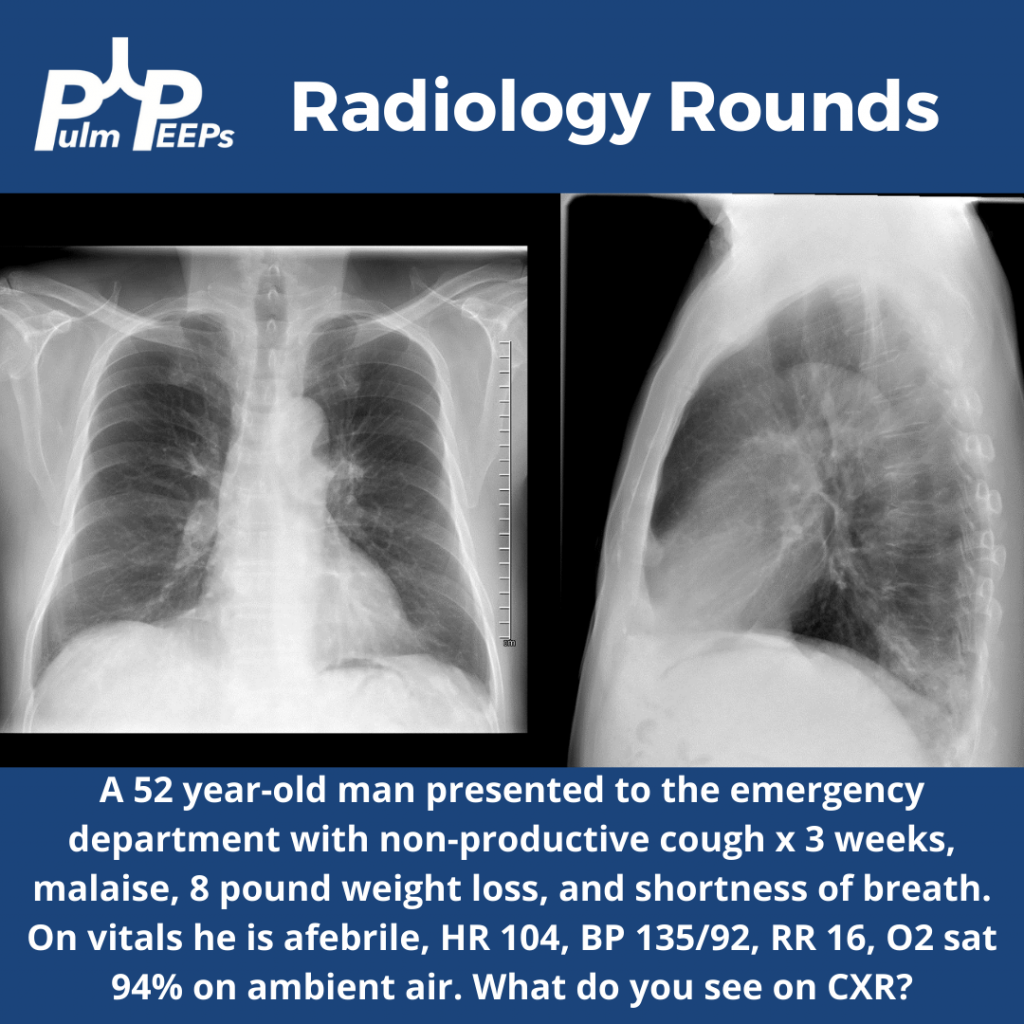
It is Tuesday and time for another #RadiologyRounds!! This is a patient who presented to the emergency department with symptoms of cough, dyspnea, malaise, and weight loss. A PA and lateral CXR was obtained.
Time for another #RadiologyRounds!! This week we’re looking at the coronal CT scan views, which can be extremely helpful and are often under-utilized. Follow us on Twitter to work through Radiology Rounds cases as they come out.
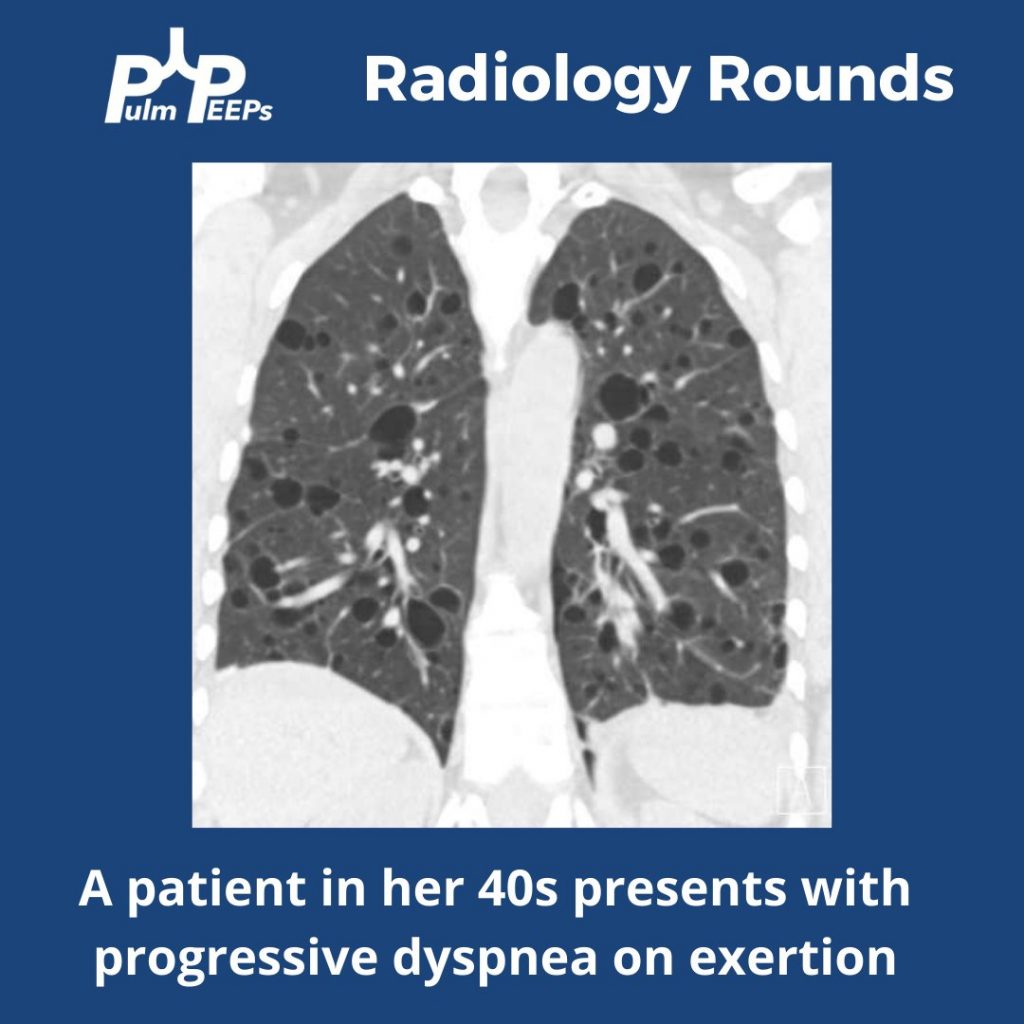
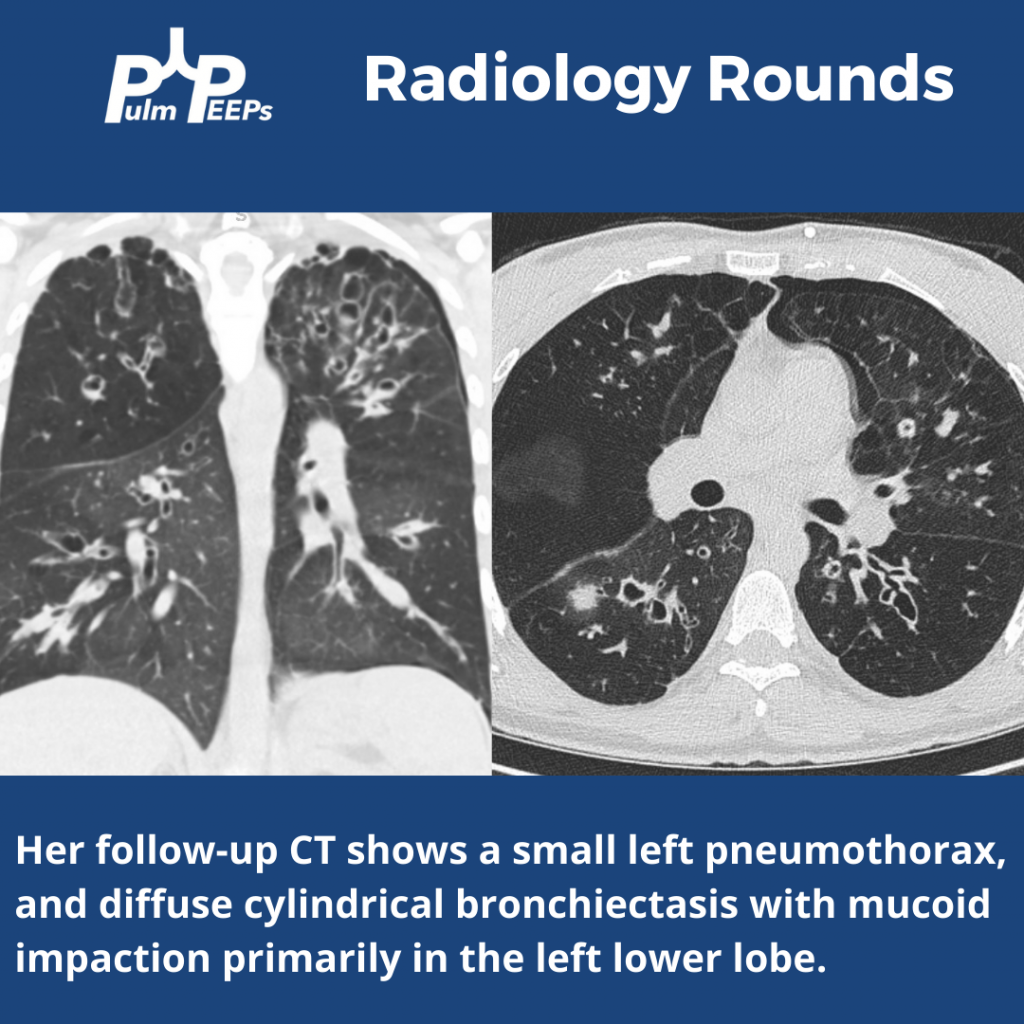
Our patient had an elevated VEGF-D level, a renal angiomyolipoma identified on CT abdomen, and imaging with diffuse cystic lung disease confirming her diagnosis of LAM. Make sure to check out the ICUOnePager made by Dr. Nick Mark.
This week’s #RadiologyRounds is brought to you by our newest Contributor, Matthew Tsai! Matt will be continuing to work with us to bring you great cases and images and we are thrilled to have him on the team! Follow us on Twitter and Instagram for our Radiology Rounds, podcast episode releases, and more!
This week on #RadiologyRounds we are extremely excited to share a case brought to you by one of our new Associate Editors, Leon Mirson! Enjoy, and follow us on Twitter and Instagram for content delivered to you weekly!
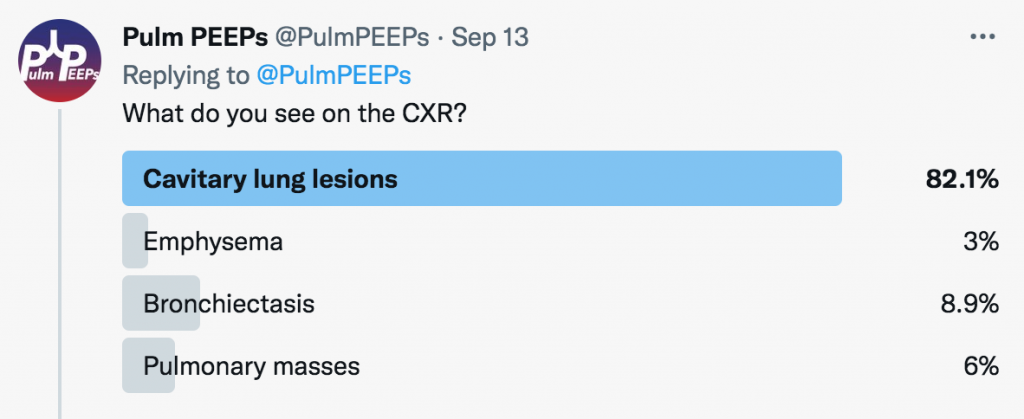
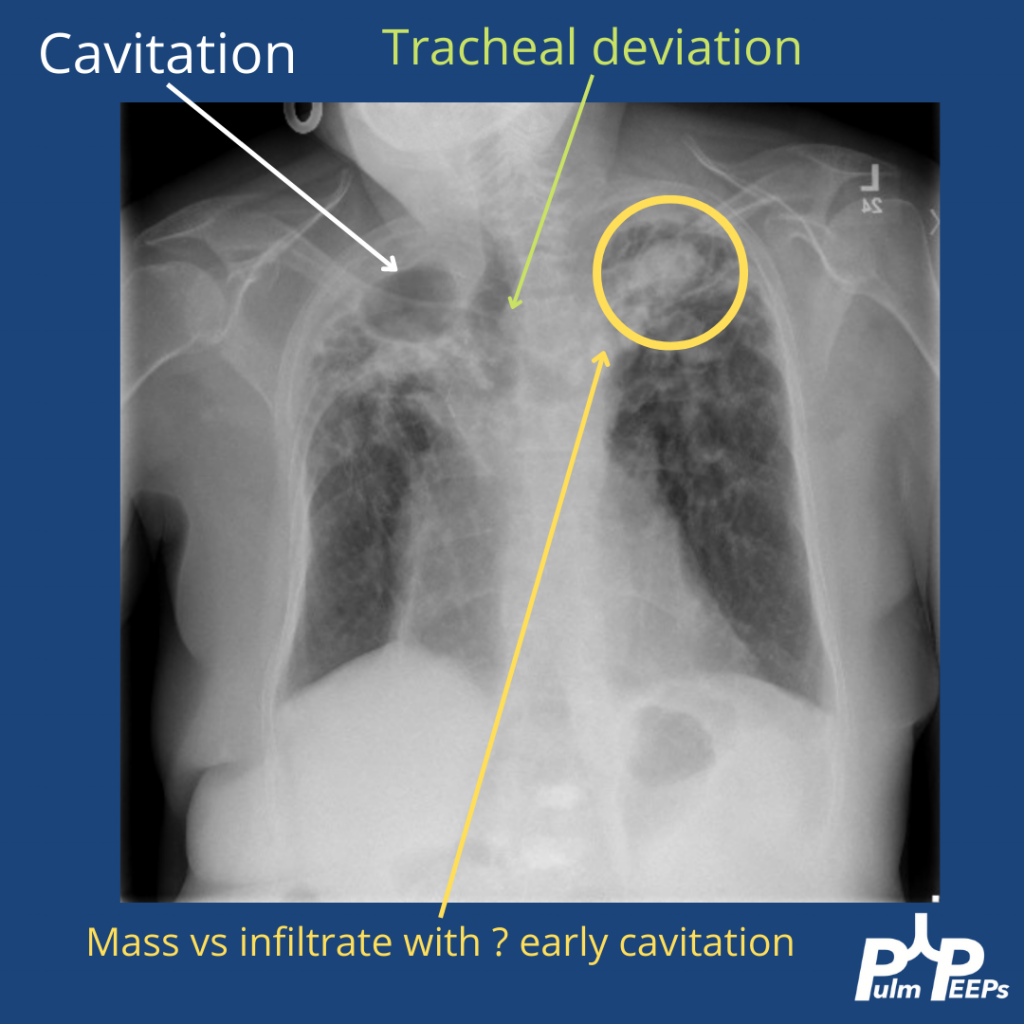
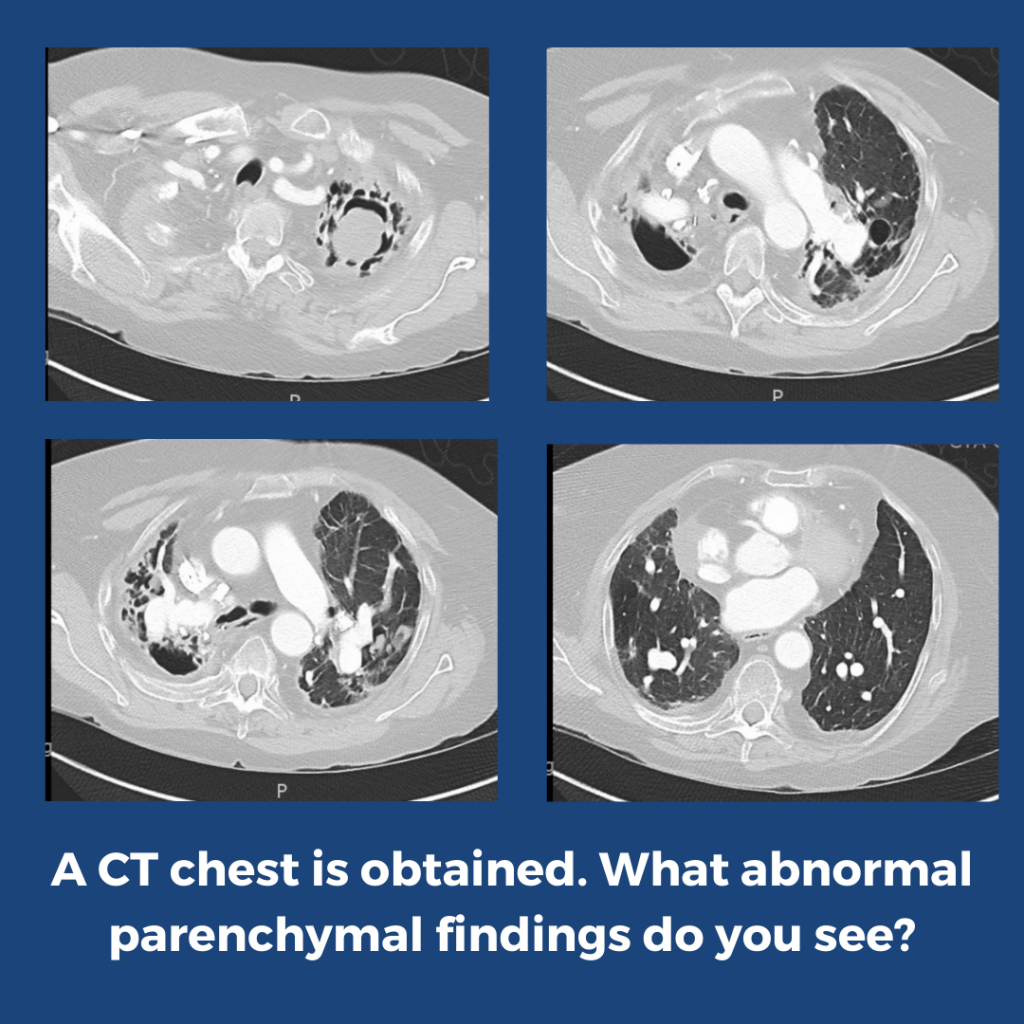
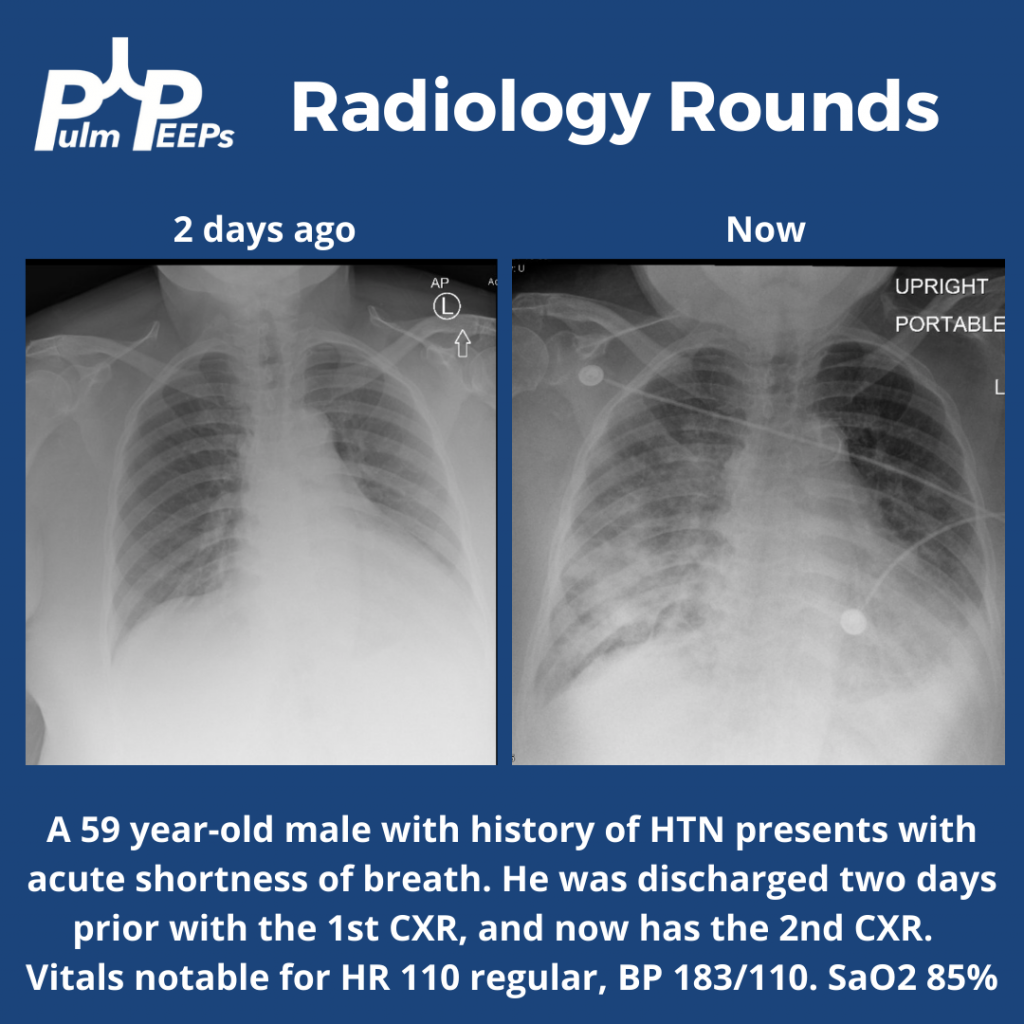
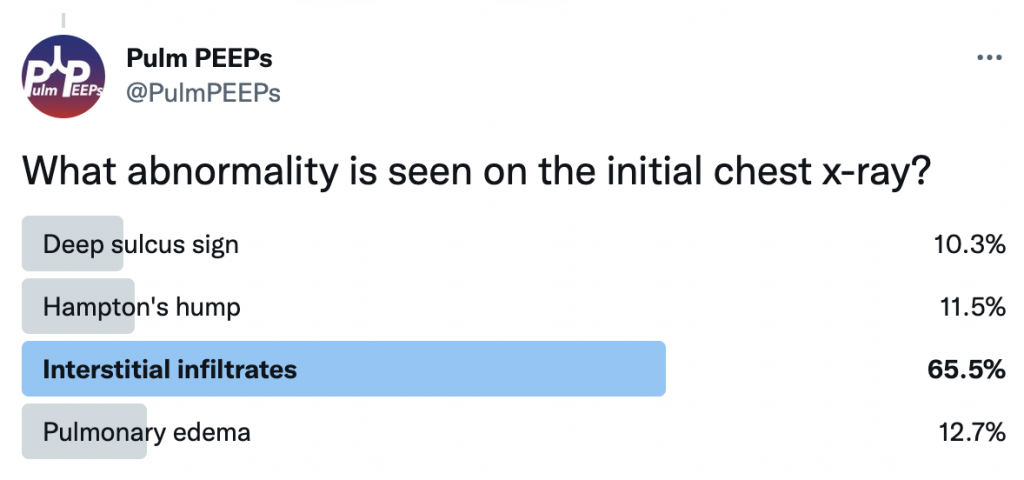
What abnormalities do you see on this CXR to help explain the patient’s presentation?
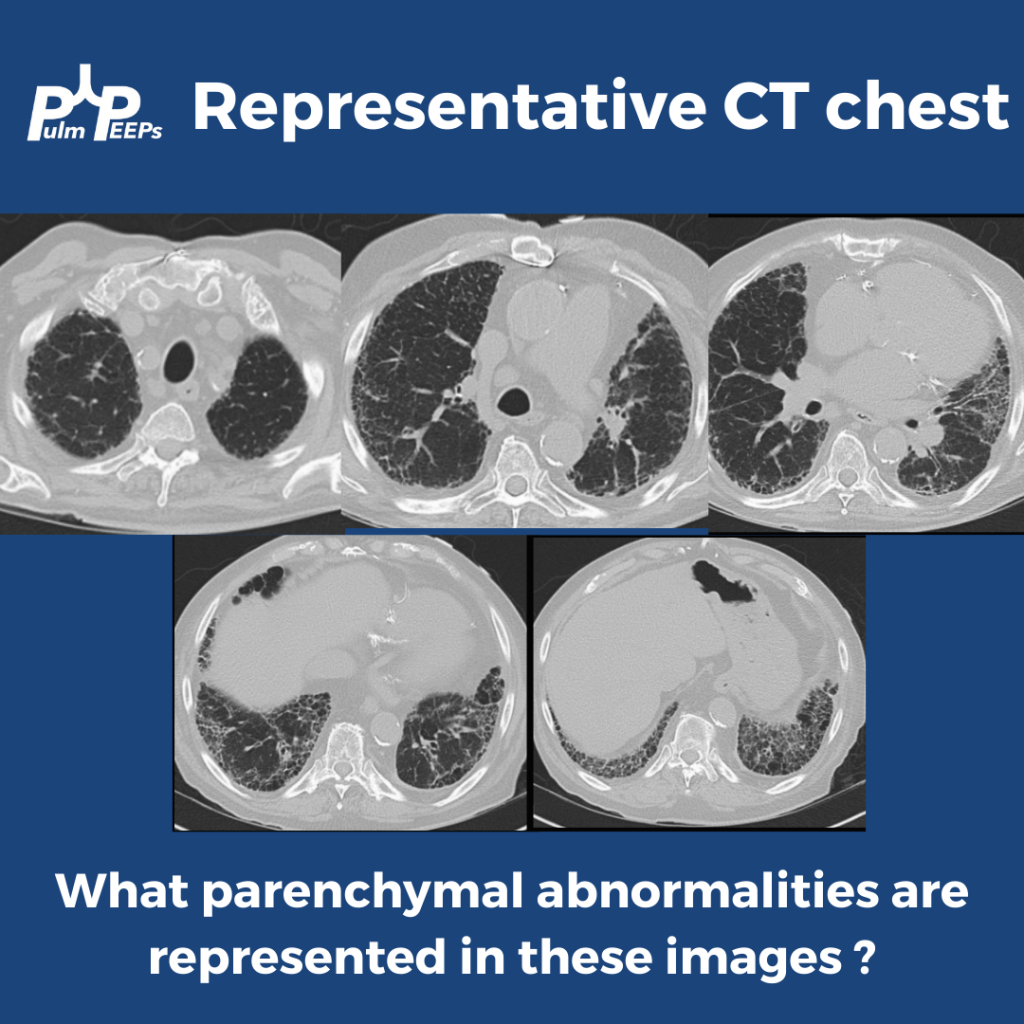
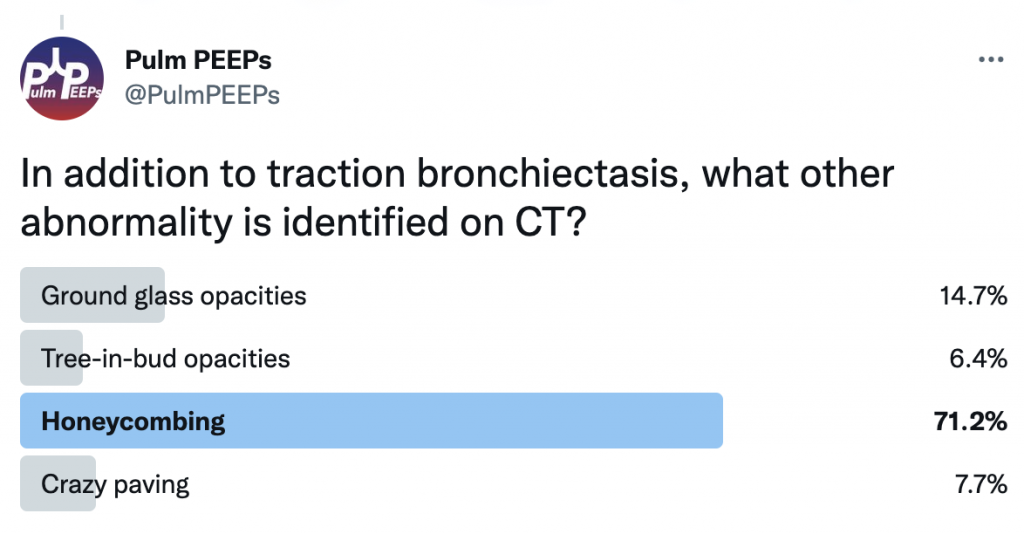
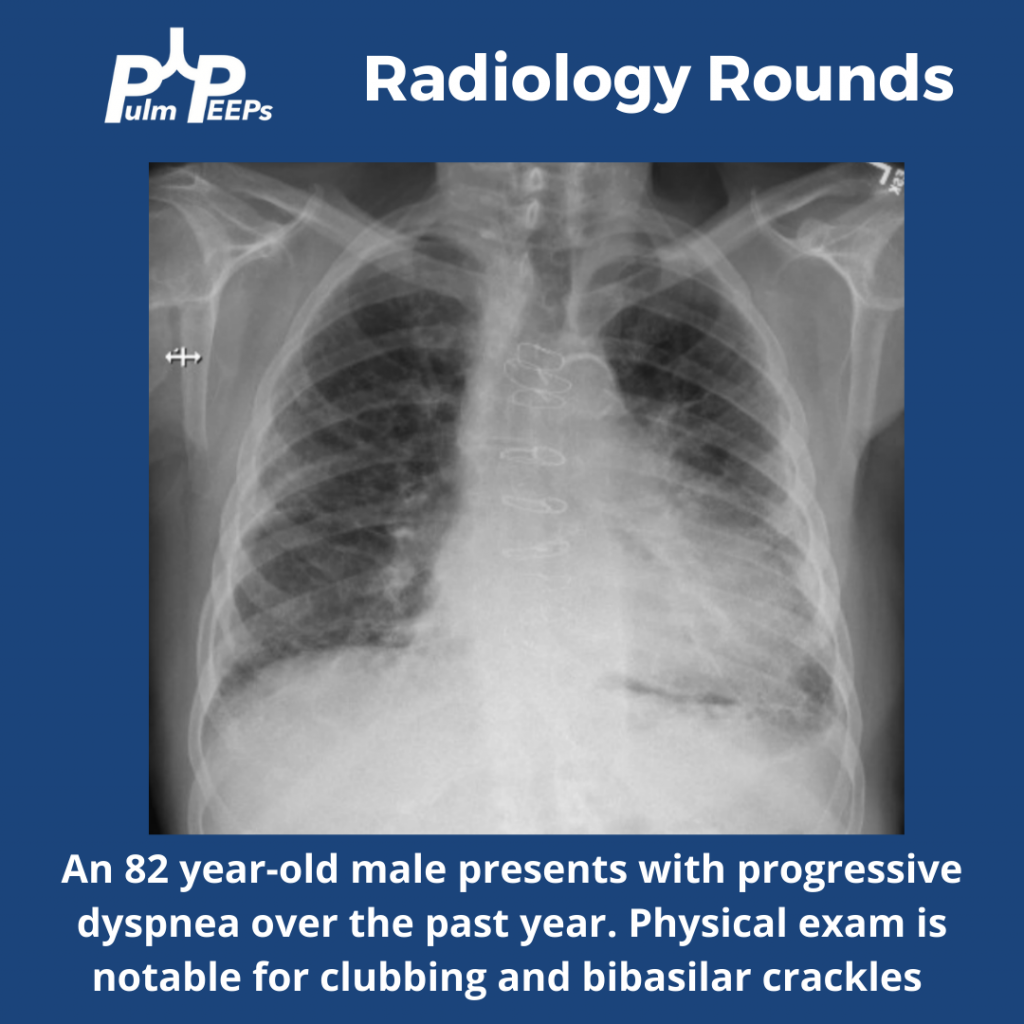
The CT scan has reticular changes consistent with interstitial lung disease and there are multiple features that help us define the pattern of the ILD. His CT notably has very few ground-glass opacities, there is traction bronchiectasis, and honeycombing with a basilar and peripheral / sub-pleural predominance.
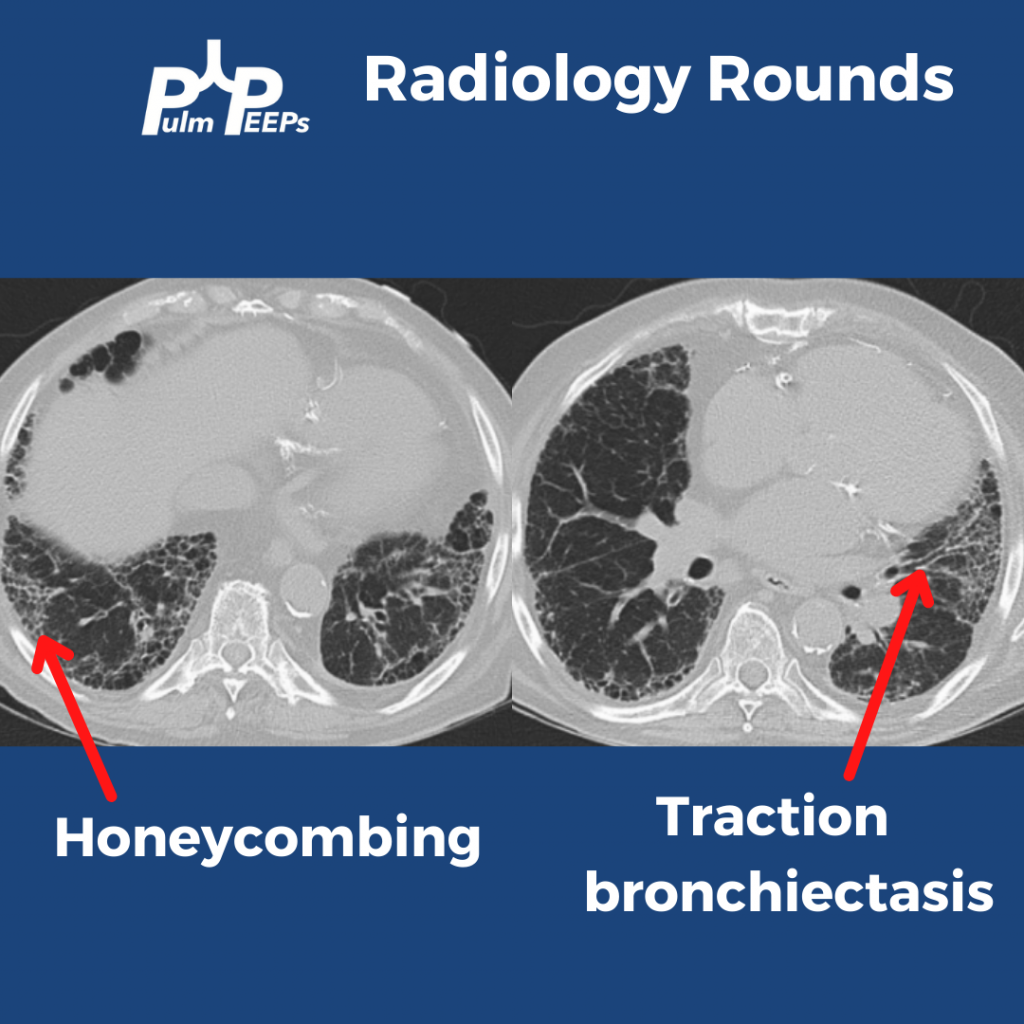
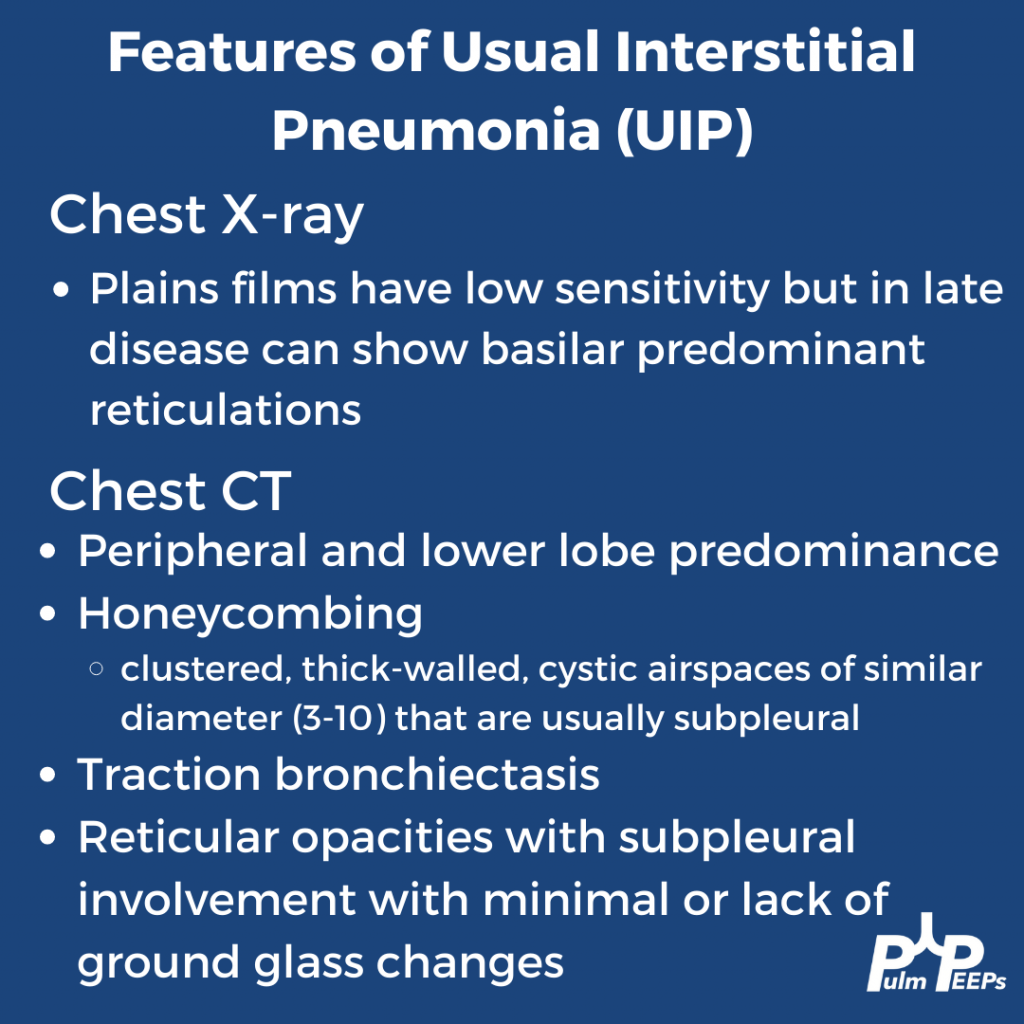
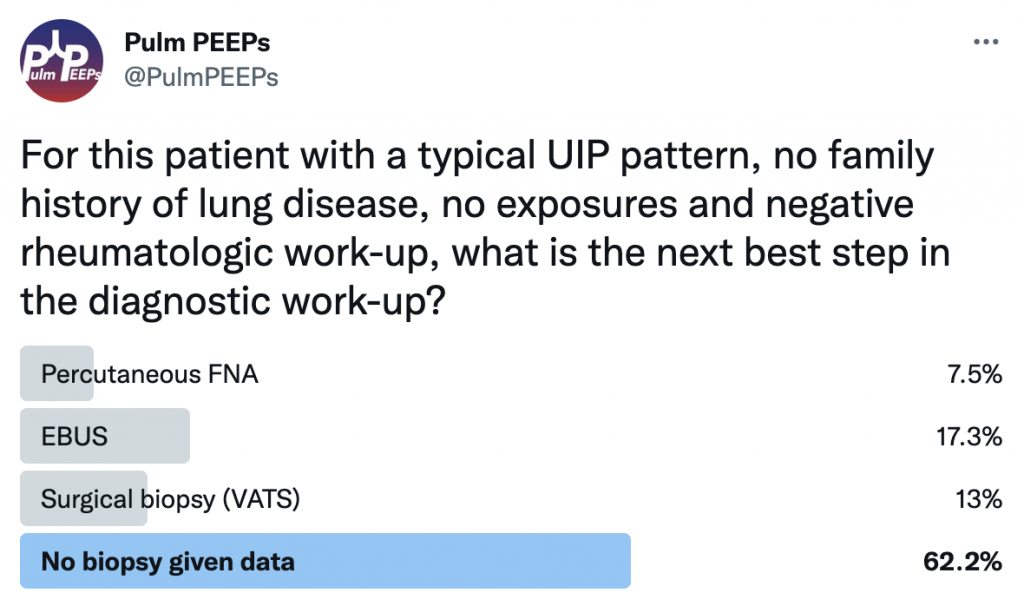
Taking all these features together, the patient’s radiographic presentation is consistent with Usual Interstitial Pneumonia (UIP)
This patient had a thorough history taken and he had no prior smoking and no occupational or environmental exposures of significance. He had no family history of interstitial lung disease. A broad history was taken regarding symptoms of connective tissue disease and a broad serologic workup was sent, all of which were unremarkable. What would you want to do next diagnostically?
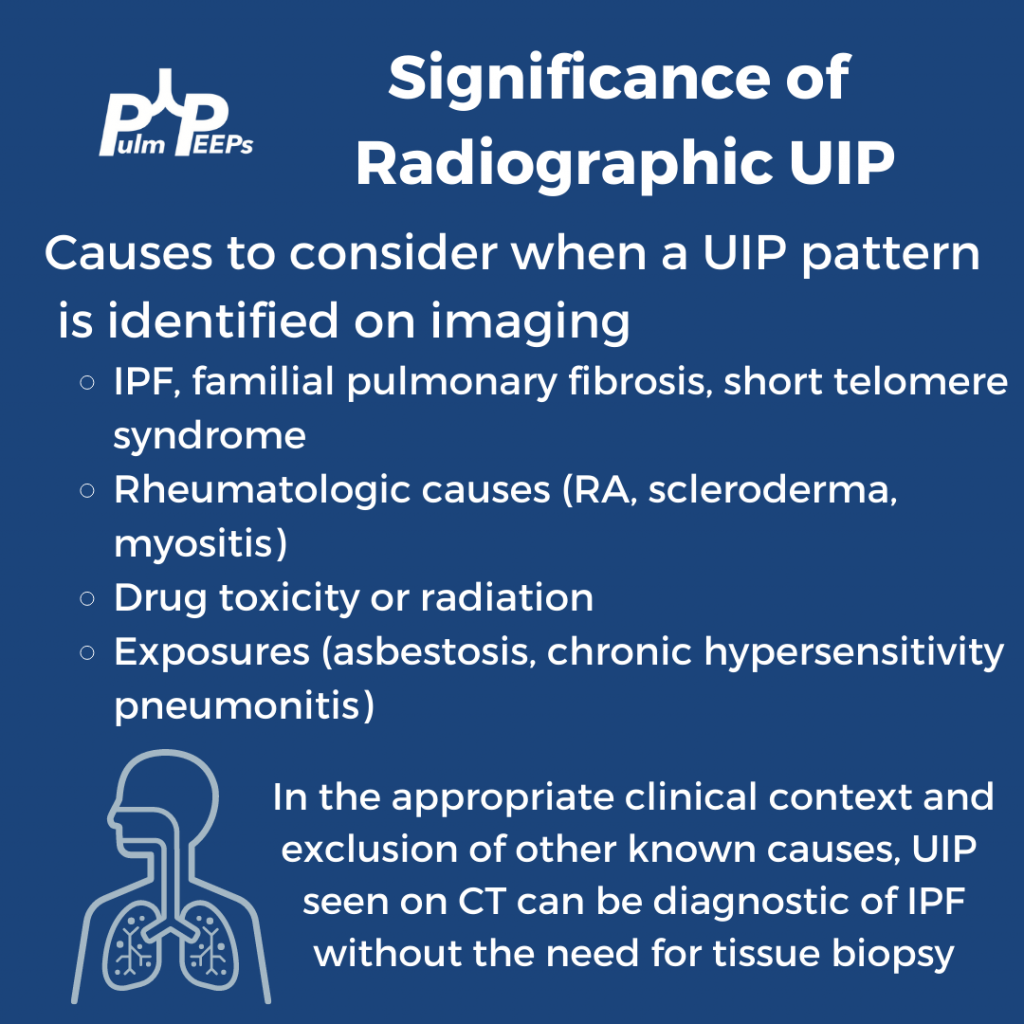
If you want to learn more about diagnosing interstitial lung disease, listen to our prior Top Consults episode on diagnosing ILD with experts in the field and see these prior #RadiologyRounds on Fibrotic NSIP and Sarcoidosis.

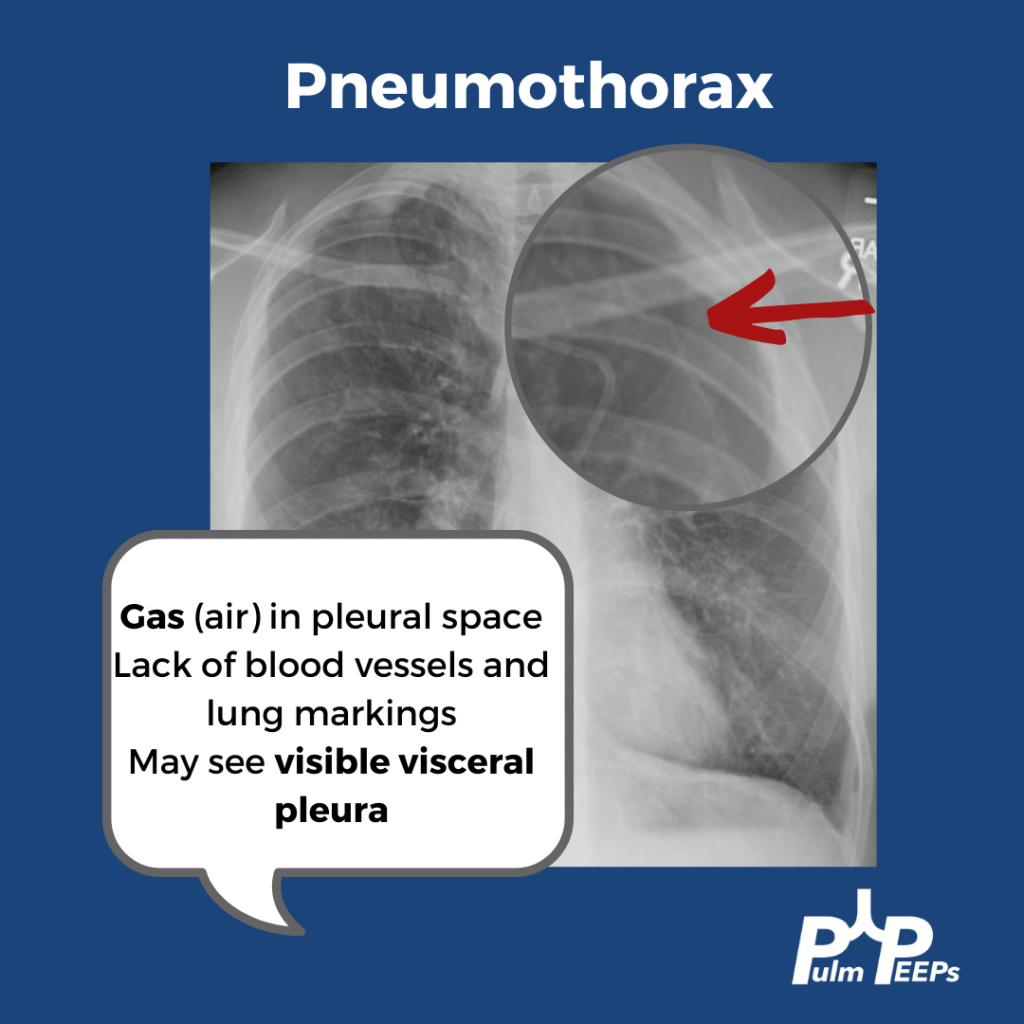
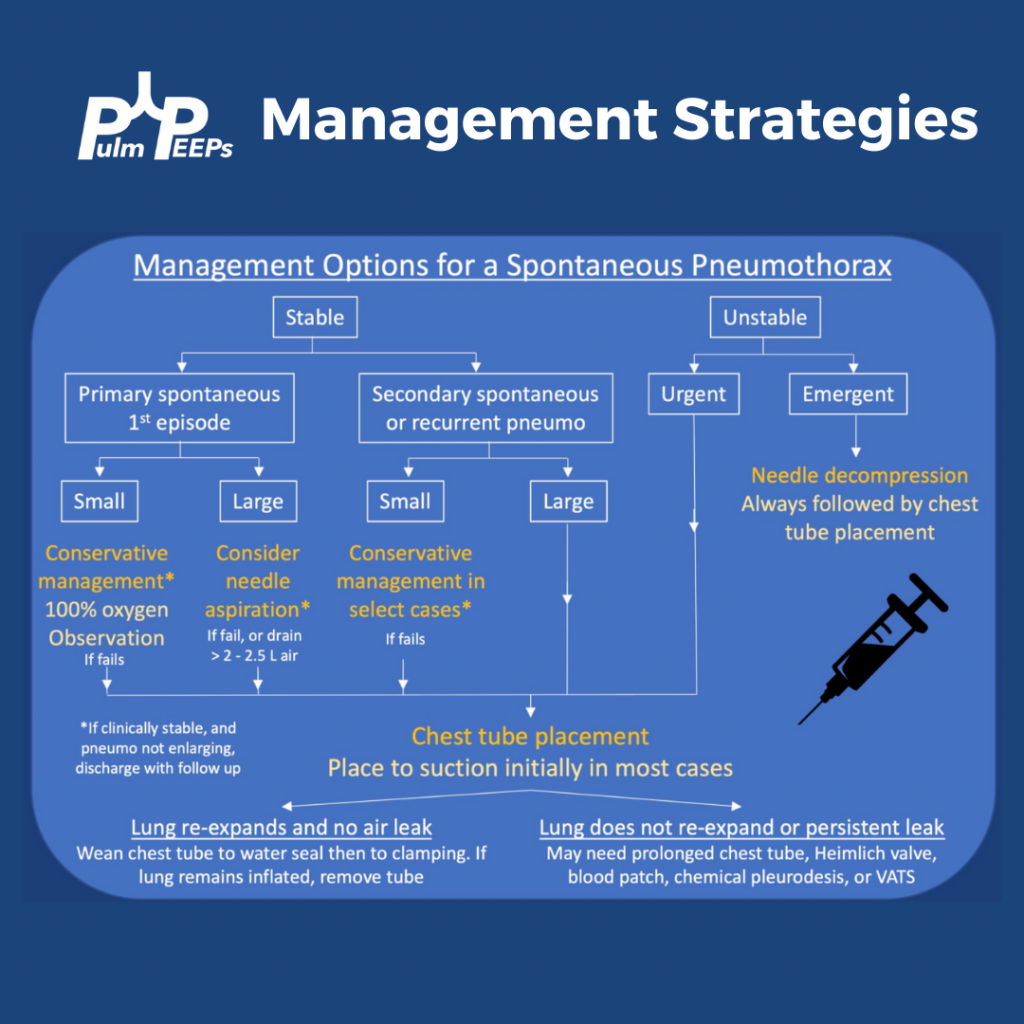
We are excited to bring you another #RadiologyRounds which applies some of the knowledge from our most recent episode on pneumothorax.
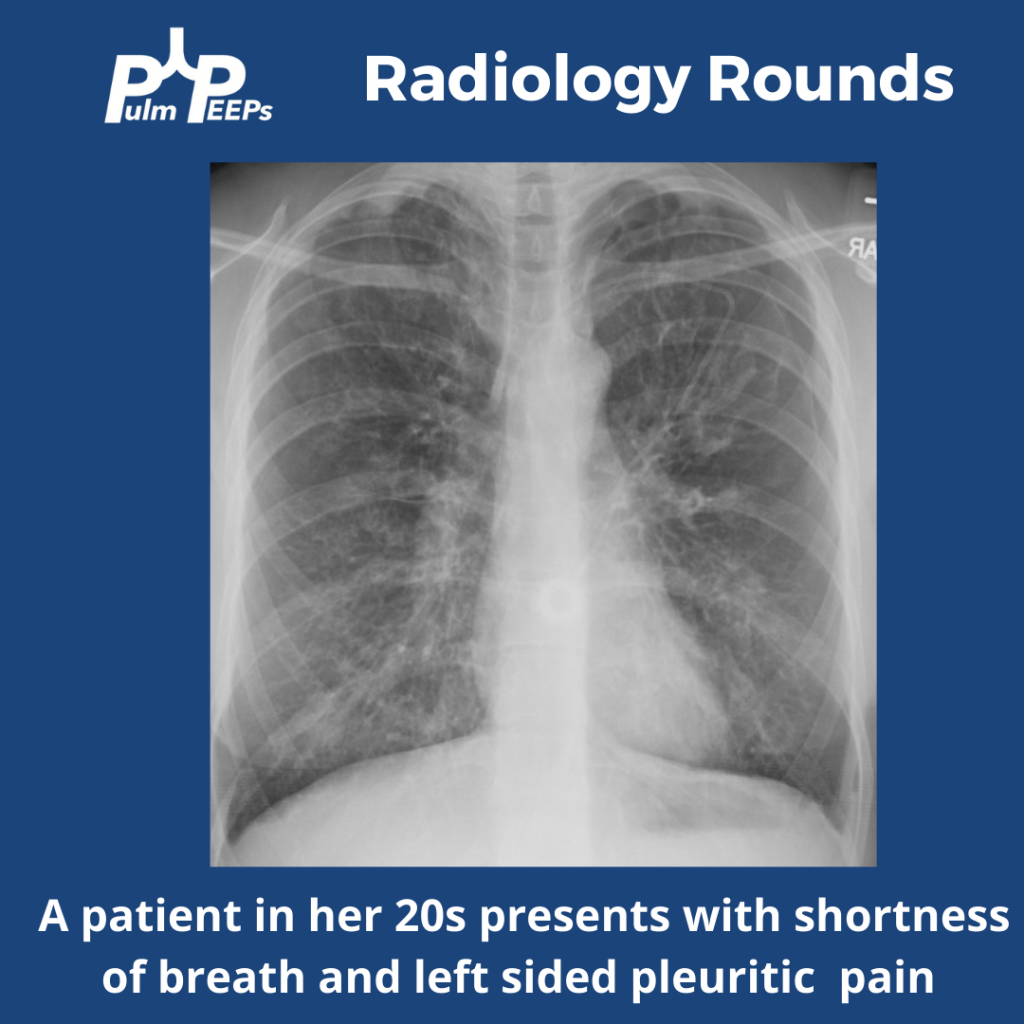
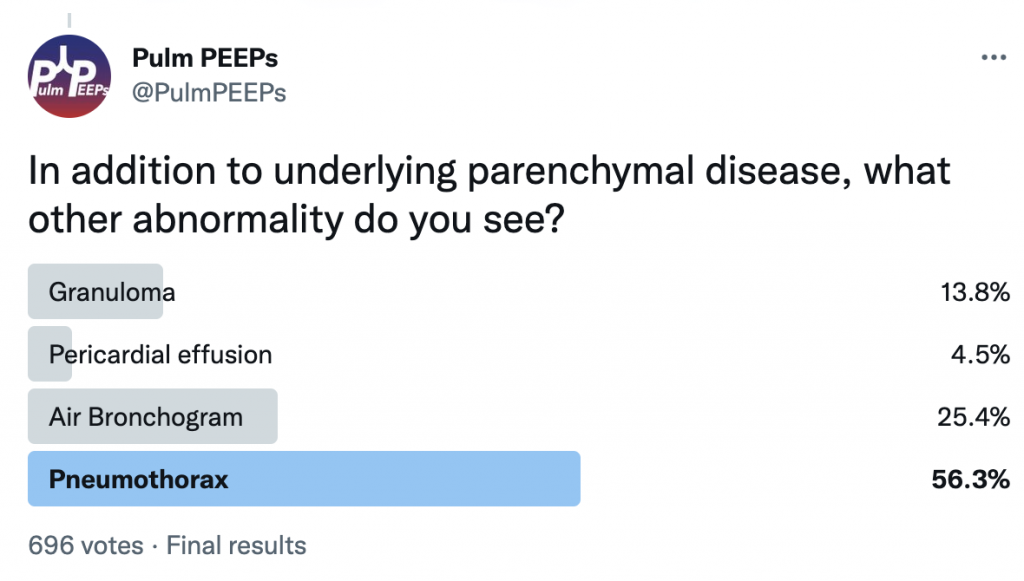
She is presenting with a 1.5 cm left pneumothorax. You can see lucency representing air in the pleural space. There are a lack of blood vessels or lung markings extending to the periphery and you can see the visceral pleura.
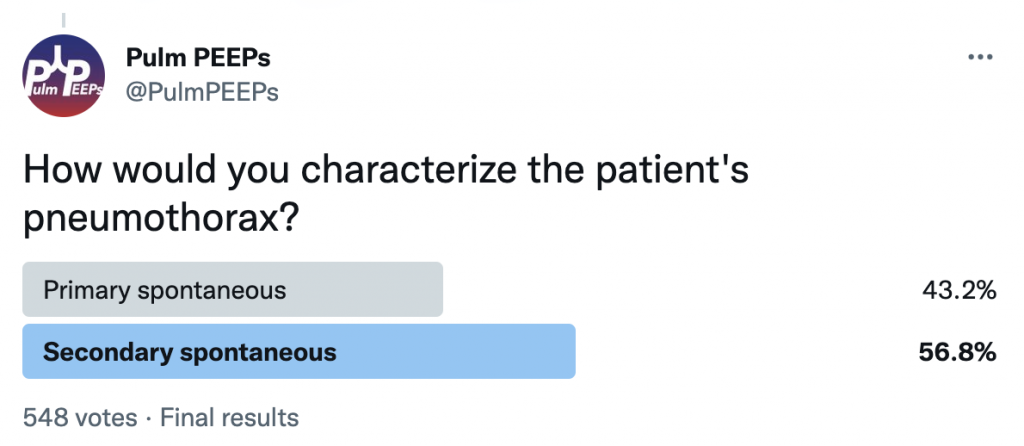
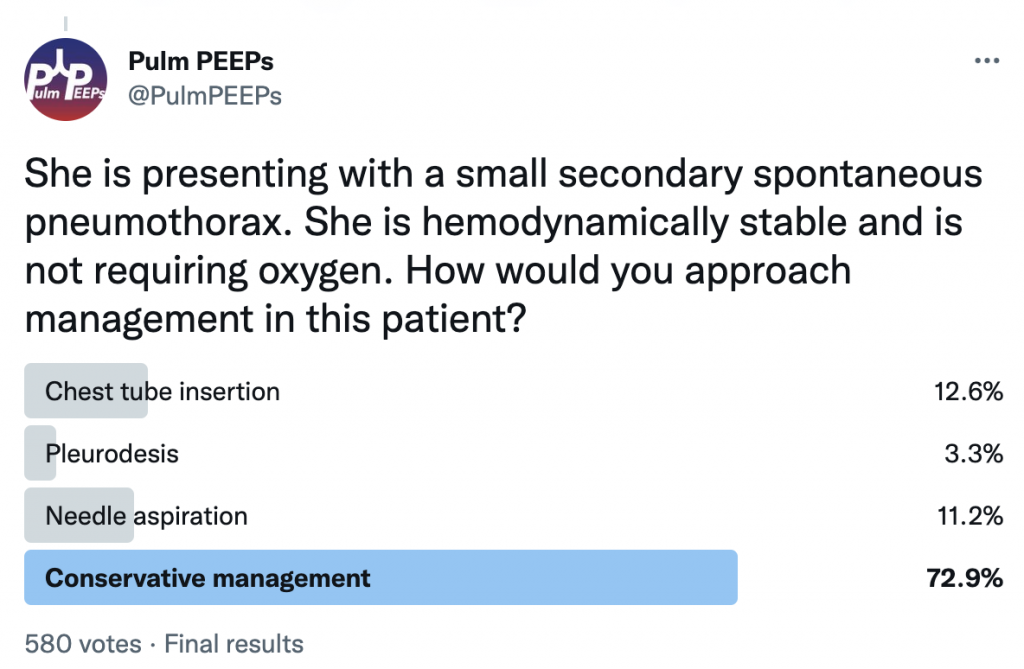
She is presenting with her first pneumothorax which is a small, spontaneous pneumothorax secondary to her underlying cystic lung disease. She was managed conservatively and followed closely outpatient with ultimate resolution of her pneumothorax.
This week on #RadiologyRounds we have a patient with some key clues on the initial X-ray that help lead to the ultimate diagnosis.
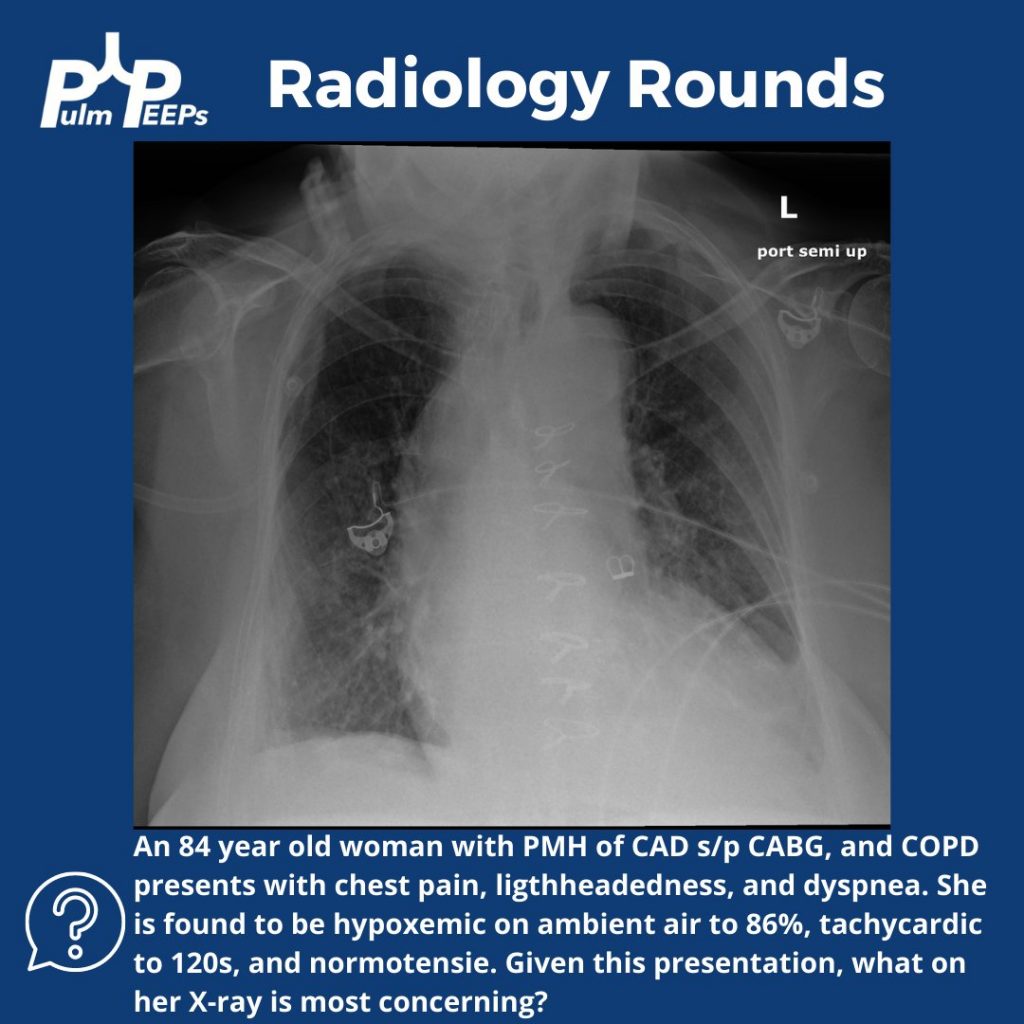
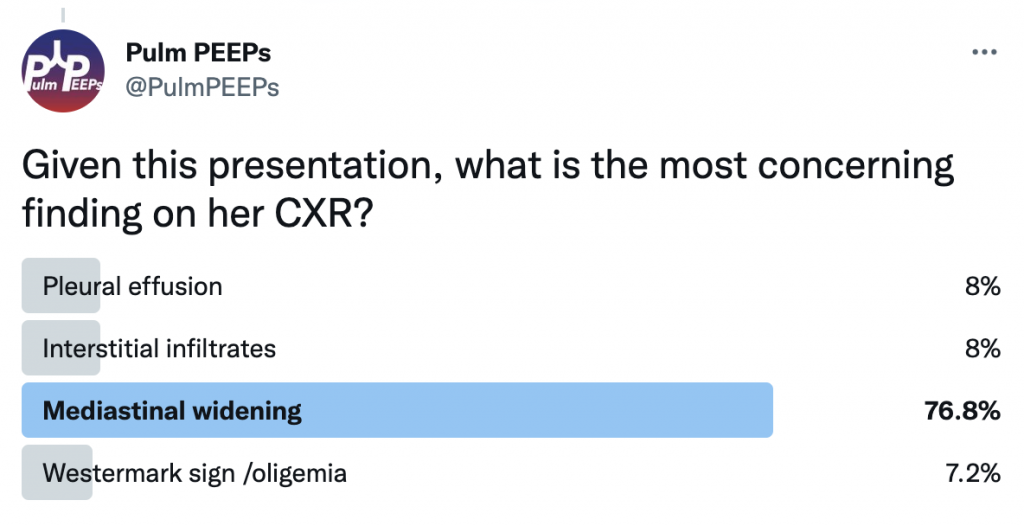
While the patient has multiple findings on the X-ray, the mediastinal widening is the most concerning finding in the setting of acute chest pain, shortness of breath, and lightheadedness.
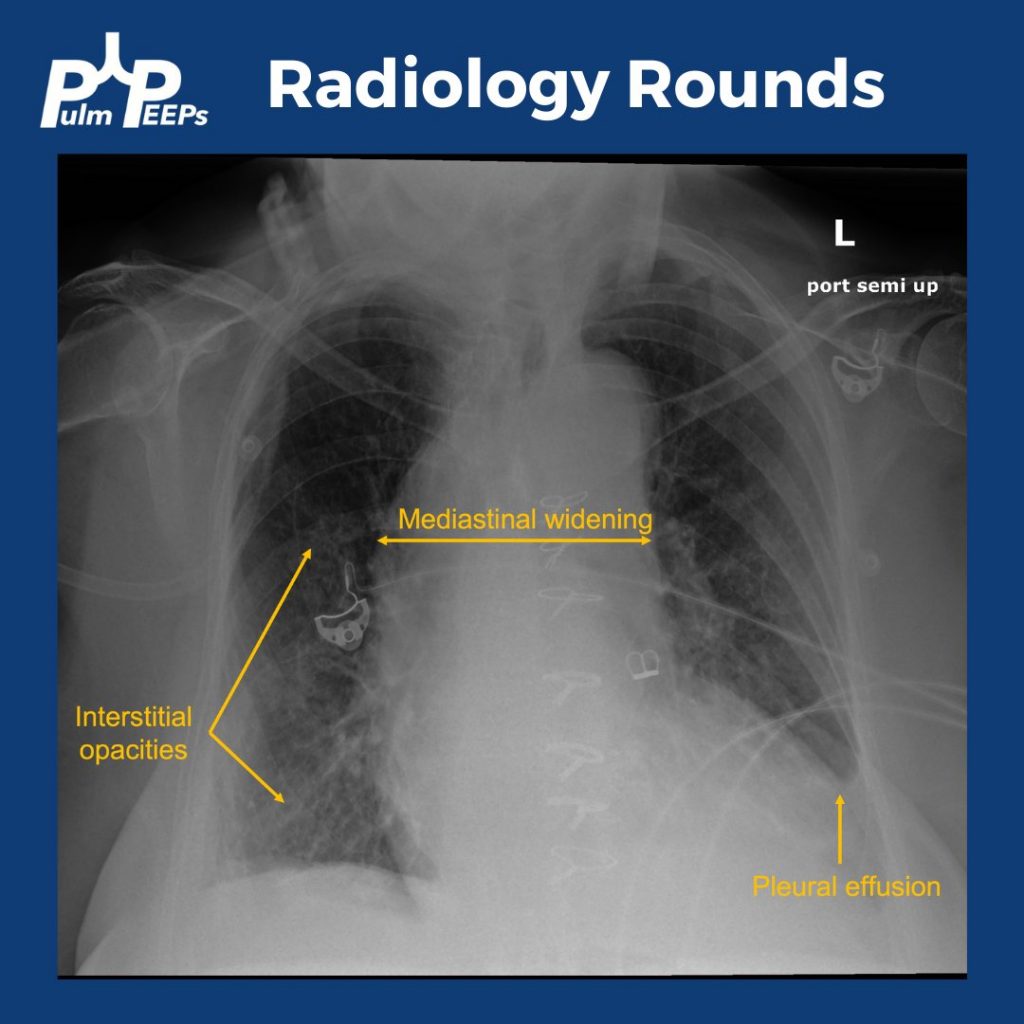
Mediastinal widening has a broad differential, which includes some can’t miss and life-threatening diagnoses
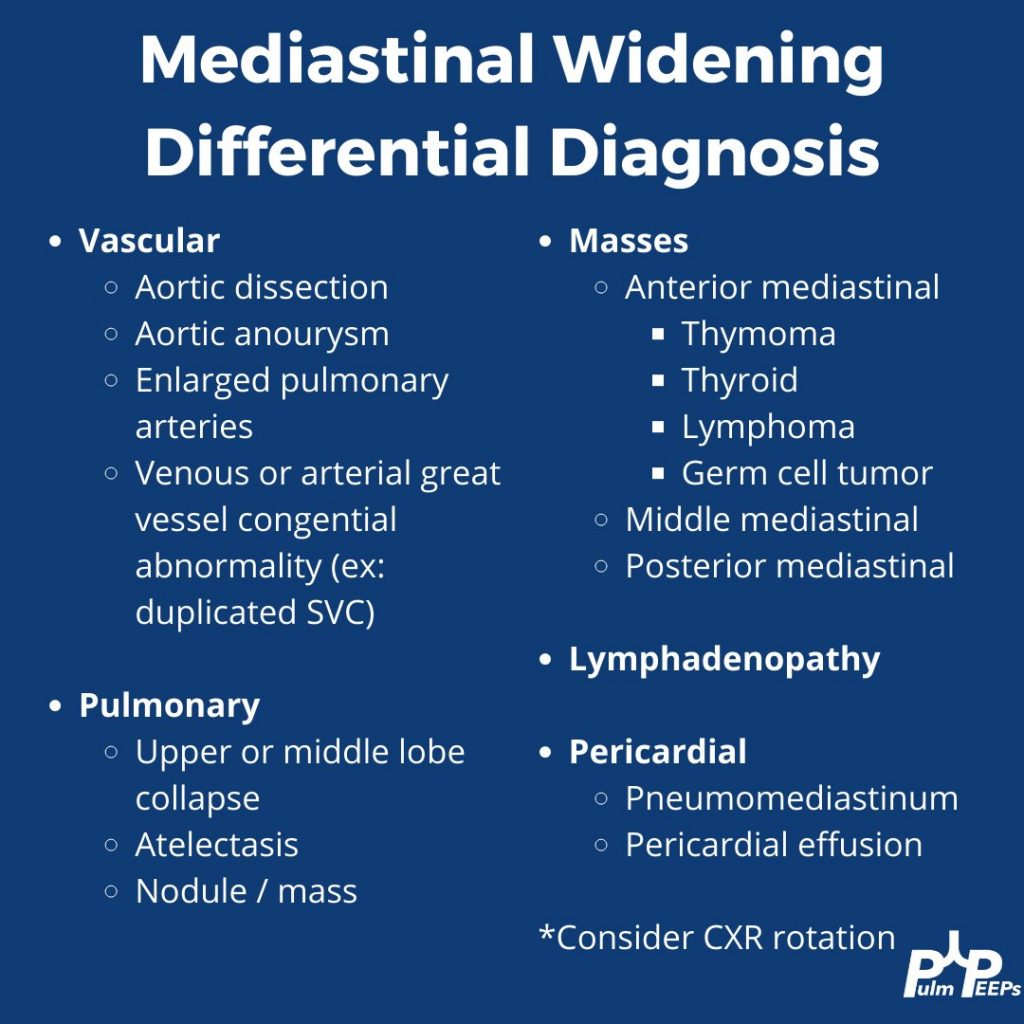
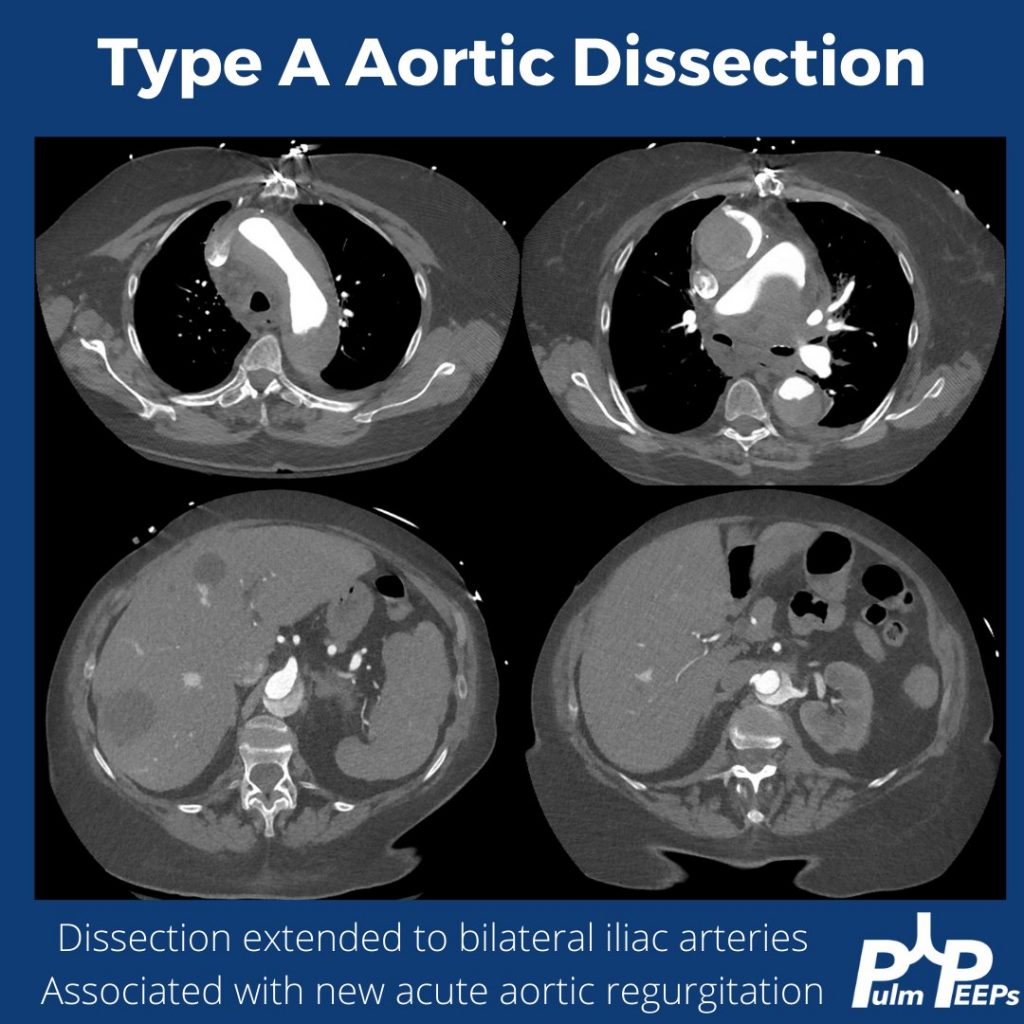
The key point is that aortic dissection, or ruptured thoracic aortic aneurysm, is high on the differential for this patient. Cross-sectional imaging is warranted and should be timed appropriately to evaluate the aorta. A triple rule-out CT would accomplish this as well. This patient had a CTA of the chest and was found to have a large type A aortic dissection with significant extension.
This week on #RadiologyRounds we continue our series on COPD. Make sure to listen to all our episodes made in collaboration with the ATS Clinical Problems Assembly.
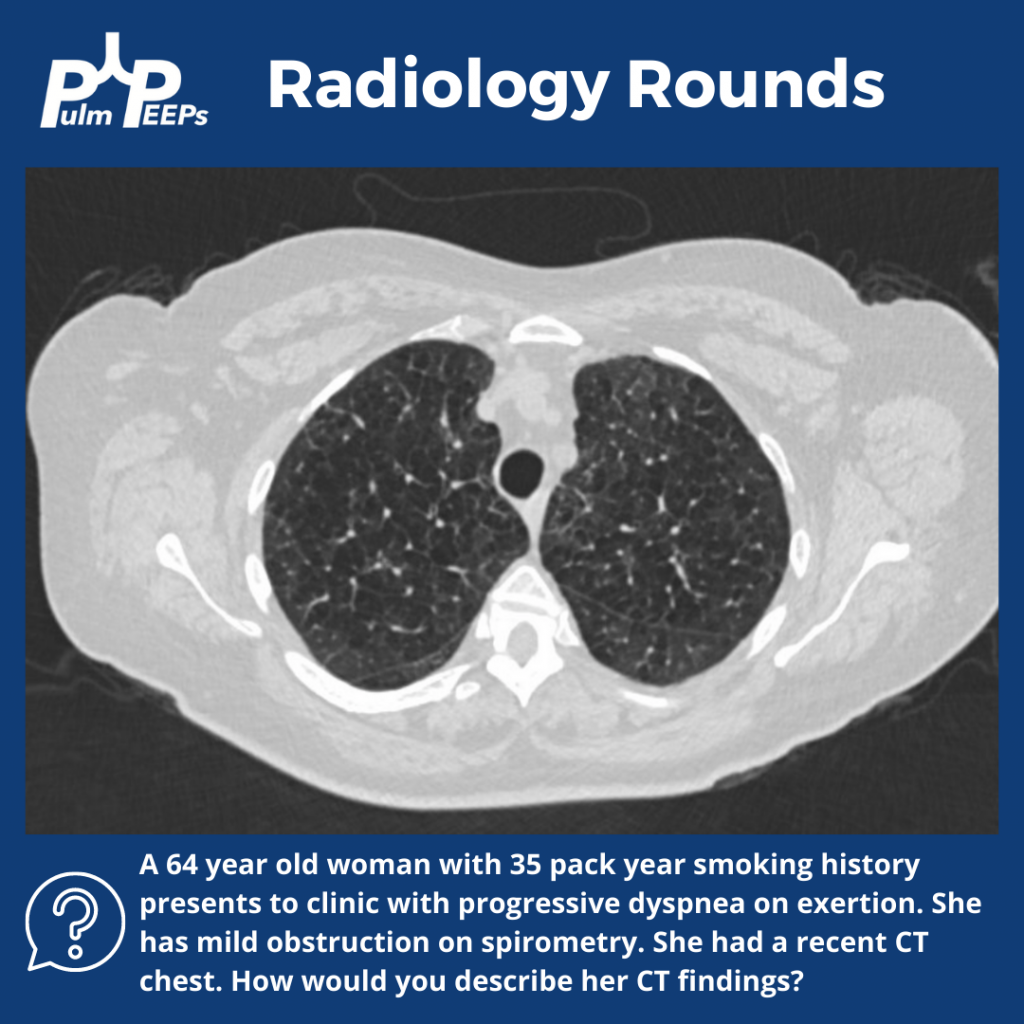
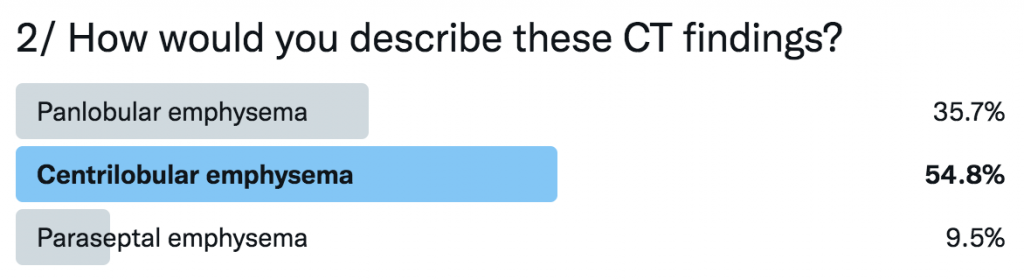
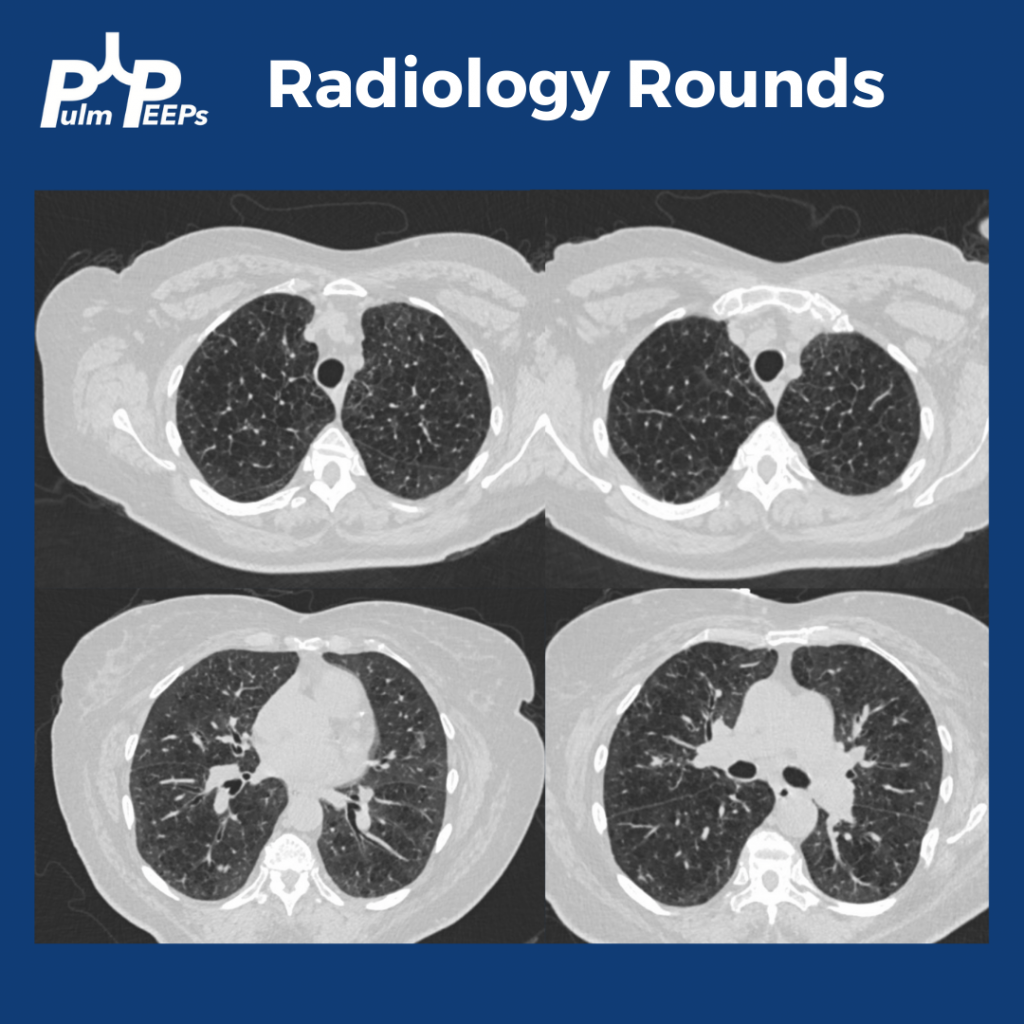
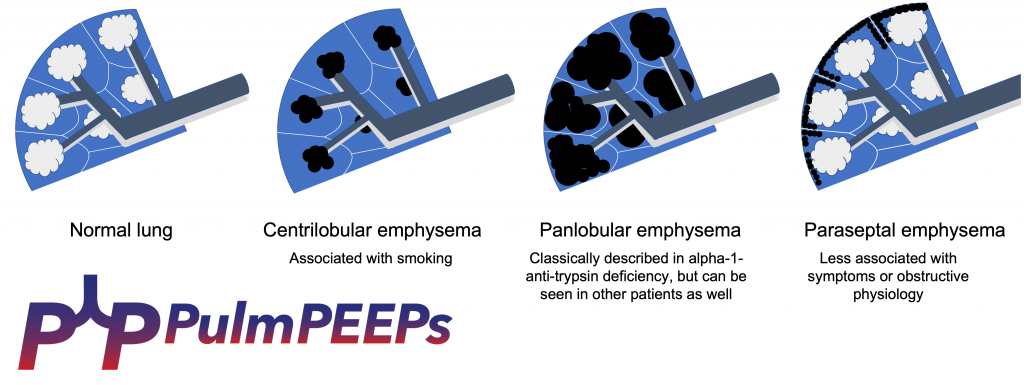
The CT shows moderate to severe centrilobular emphysema. These different patterns of emphysematous changes on CT can be related to the underlying driver of the disease and to symptom and disease severity.
In terms of follow-up, would you test this patient for alpha 1 anti-trypsin deficiency?
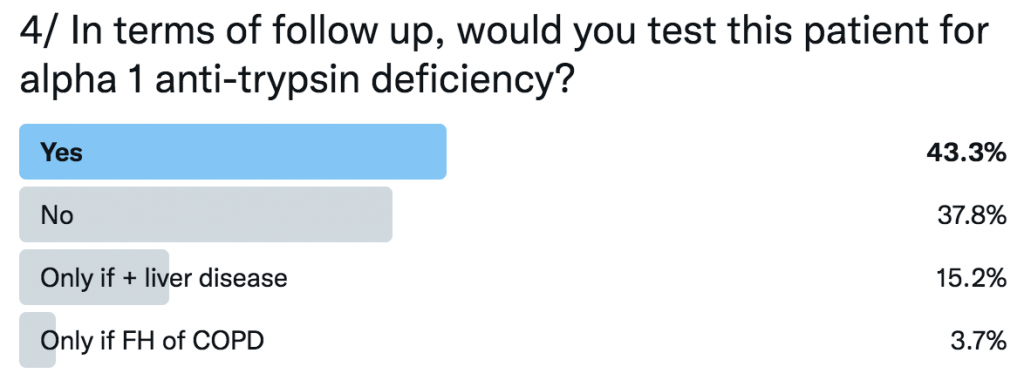
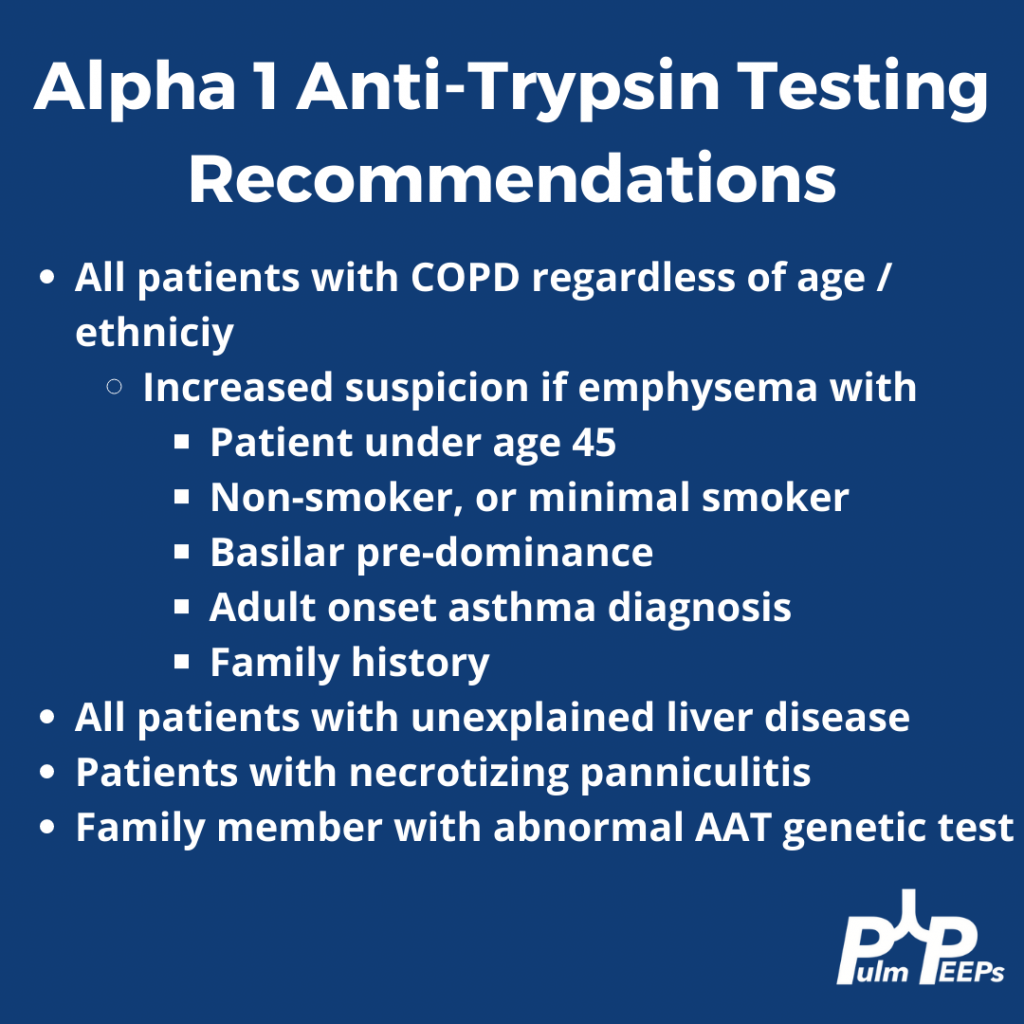
Current GOLD guidelines recommend that everyone with COPD, regardless of age or ethnicity should be tested for alpha 1 anti-trypsin deficiency.