We are thrilled today to be previewing CHEST 2023! The Annual Meeting is taking place October 8th – 11th in Honolulu, Hawaii, and we are joined today by CHEST enthusiasts and the past, present, and future conference chairs. Listen now to hear what is in store for you next month in Hawaii, to plan your conference experience, and find out what sessions are can’t-miss!
Meet Our Guests
Aneesa Das is a Professor of Medicine at The Ohio State University Wexner Medical Center. She is the Assistant Director of the OSU Sleep Program and the Director of the Portable Sleep Testing Program. She was the Vice-Chair of the CHEST 2022 Scientific Programming Committee, and the Chair for 2023
Subani Chandra is an Associate Professor at Columbia University. She is the Vice Chair of Medicine for Education, and the internal medicine residency program director. She was the chair of the CHEST Scientific Program Committee for CHEST in 2022 and joined us when we came to you live from Nashville last year. Subani is currently the Chair for the Training and Transitions Committee for CHEST.
Gabe Bosslet is a Professor of Clinical Medicine in the Department of Pulmonary, Critical Care, Sleep and Occupational Medicine at Indiana University. He is the Assistant Dean for Faculty Affairs and Professional Development at IU. He is the current Vice Chair of the CHEST 2023 Scientific Programming Committee and the Chair Elect for CHEST 2024.
Huzaifah Salat is a budding clinician educator who is currently working as a consultant pulmonologist and intensivist at Advocate Aurora Health in Wisconsin. He recently completed his Pulmonary and Critical Care Fellowship at the University of Oklahoma Health Sciences Center. He has worked with Pulm PEEPs before on some fantastic Tweetorials.
CHEST’s Local Efforts and Initiatives to Support Survivors of the Maui Wildfires
We’re excited to be back with another Fellows’ Case Files. Today, we’re visiting the University of Pittsburgh to meet a fantastic fellow and a dedicated educator, and to hear about a fascinating case. Let us know if you’ve ever had a similar case, and share your interesting cases with us!
Meet Our Guests
Rachel Wojcik obtained her B.S. in Biology from Mercyhurst University and a Master’s in Liberal Studies from the University of Denver in Global Affairs with a focus on Healthcare. She completed her MD at the University of Colorado before completing her residency and chief resident year at the University of Pittsburgh and has continued her training at Pitt for PCCM fellowship.
Dr. Stephanie Maximous is an Assistant Professor of Medicine at the University of Pittsburgh School of Medicine and is the Clinical Education APD for the Pulmonary and Critical Care Fellowship program. She completed her fellowship at Pitt in addition to obtaining a Master’s Degree in Medical Education there. She teaches in and directs courses throughout the medical school, residency, and fellowship and was recently awarded the 2023 Outstanding Subspecialty Teaching Attending Award from the housestaff.
Case Presentation
Patient: A 70-year-old male with a history of idiopathic thrombocytopenia on chronic prednisone and a history of tobacco use disorder.
Presentation: Came to the hospital with 2-3 days of right-sided weakness and slurred speech.
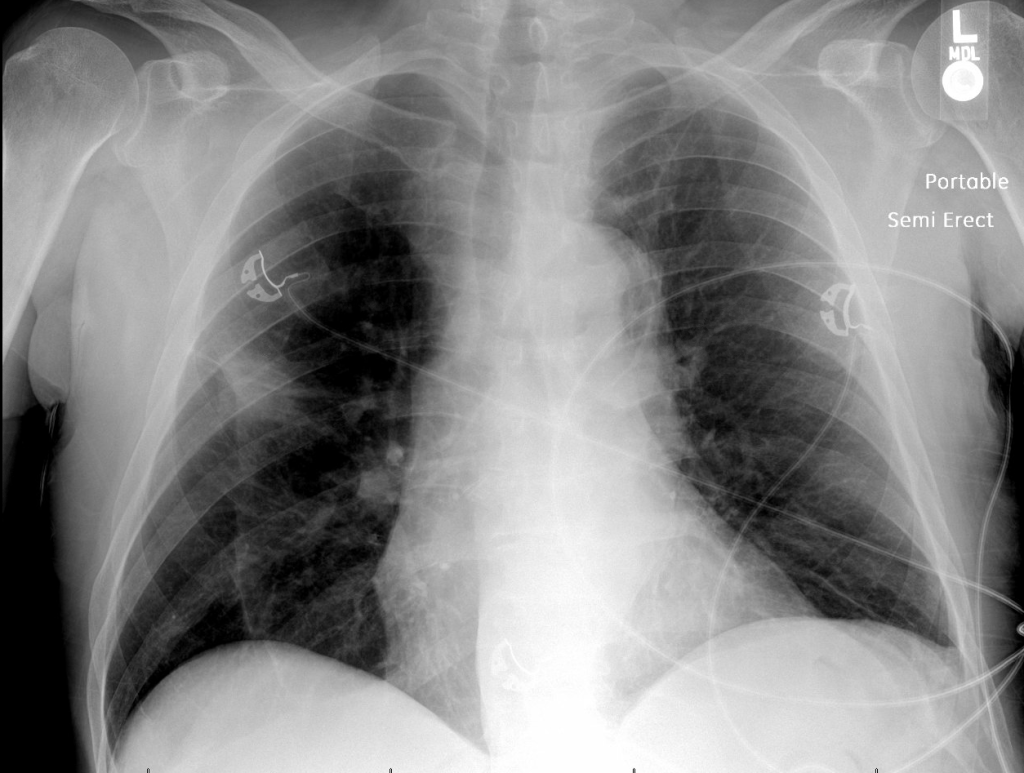
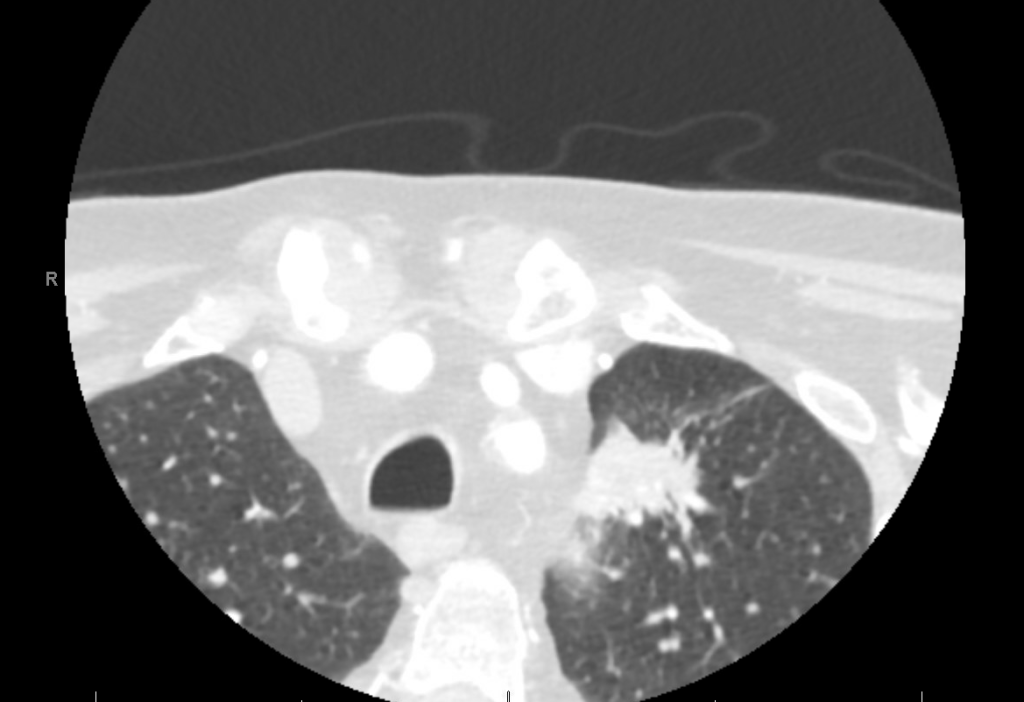
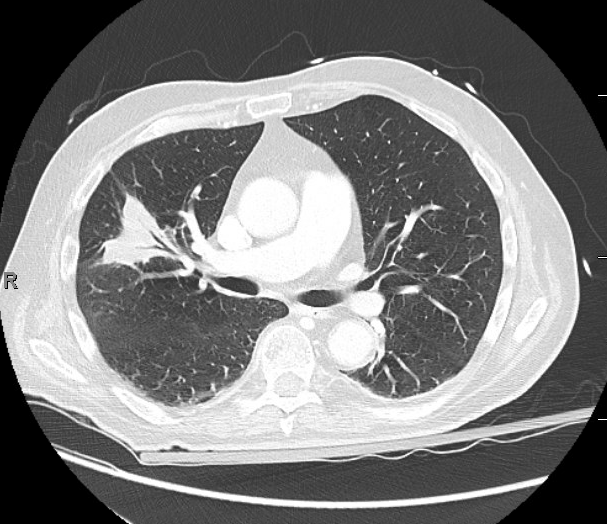
Findings: MRI showed a moderate-sized left pontine stroke. A CT angiogram of the neck showed no evidence of an occlusion, but a spiculated two-centimeter nodule at the apex of the left lung was found.
Additional Information: He requires a walker for mobility and needs help with activities like taking a shower and dressing. He had an unintentional 20-pound weight loss over six months, increased fatigue, and malaise.
Previous Investigations: A chest x-ray ordered two months prior by his hematologist was unremarkable, and a CT of the abdomen and pelvis showed no masses.
Key Learning Points
Bronchoscopy in Decision Making:
The decision to perform bronchoscopy in patients depends on a myriad of factors, including the location of any lesions, accessibility, potential risks, and the potential diagnostic yield.
Fiber optic bronchoscopy with BAL can rule out infections, and if no diagnosis is reached, more invasive methods like surgical biopsy might be necessary.
Consider the location of consolidated masses; navigational bronchoscopy might be needed for lesions without a clear airway leading into them.
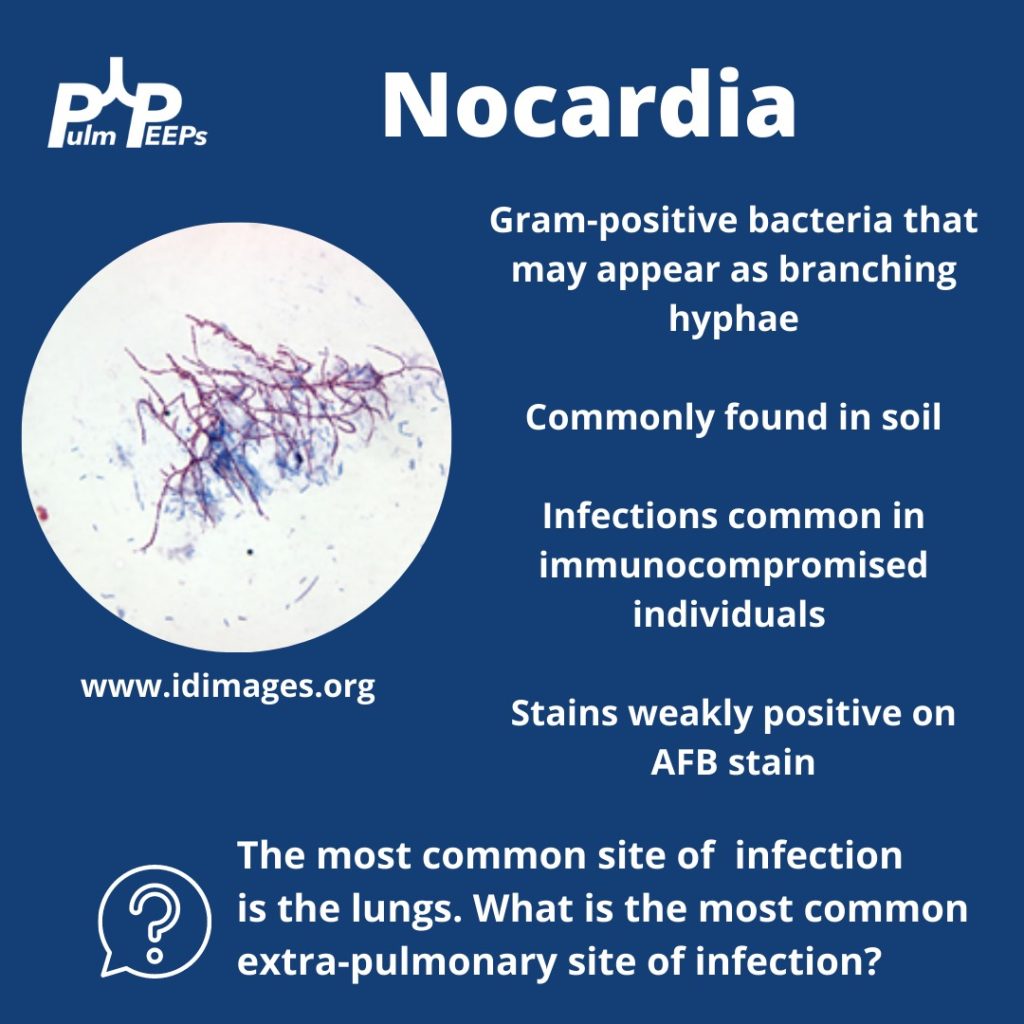
Nocardia Insights:
Nocardia is a gram-positive bacterium that stains weakly acid-fast.
It can be found in soil and certain water sources and can infect through the skin or by inhalation.
Two-thirds of patients with Nocardia are immunocompromised.
The dosage of Bactrim given for PJP prophylaxis doesn’t prevent Nocardia infections in immunocompromised individuals.
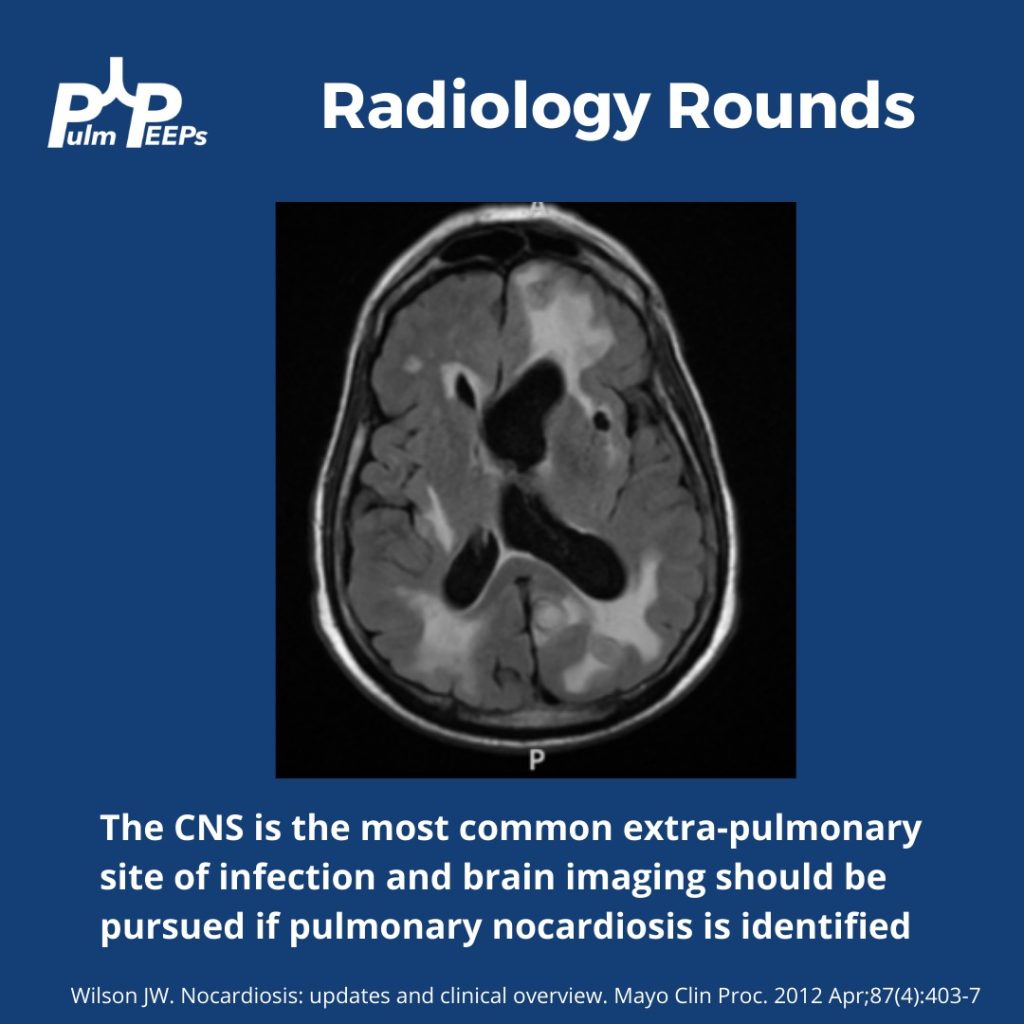
While the lungs are the most common infection site, Nocardia can manifest elsewhere, like the skin or CNS.
Treatment Approach:
Bactrim is the mainstay of treatment for Nocardia. If someone is allergic, desensitizing them can be crucial.
IV induction phases vary in length depending on the severity of the disease.
The overall treatment duration is protracted to prevent relapse.
Takeaway Points:
Bactrim for PJP prophylaxis doesn’t necessarily prevent Nocardia infections in immunocompromised individuals.
If someone is allergic to Bactrim, consider desensitizing them due to its importance in treating Nocardia.
We’re diving back into some pleural fluid today (okay that is kind of gross to think about and we apologize). If you haven’t listened to our prior pleural effusion episodes and want to start from the top, then check out Episode 36 for a general approach to pleural effusions, and Episode 37 to hear about parapneumonic effusions. Malignant effusions are another common consult question and we’ll talk about everything from detection to monitoring, to definitive management.
Meet Our Guests
Dr. David DiBardino is an Assistant Professor of Medicine at the University of Pennsylvania Medicine and is the Associate Director for Clinical Research within the Section of Interventional Pulmonology. He is also the Program Director for the Interventional Pulmonary Fellowship there.
Dr. Jamie Bessich is an Assistant Professor of Medicine and Cardiothoracic Surgery at NYU Grossman School of Medicine. She is the Section Chief of Interventional Pulmonology and is the Director of Bronchoscopy at Tisch Hospital.
Dr. Van Holden is an Associate Professor of Medicine at the University of Maryland School of Medicine and is the Pulmonary and Critical Care Fellowship Program Director there. She was last on the show for our very first Fellows’ Case Files when we discussed a fascinating case of pulmonary alveolar proteinosis.
Case Presentation
The page: 72M smoker, new effusion, concern for malignancy, tap?
Further history: 72 year old man with PMH of GOLD B COPD, tobacco use (55 pack years), HTN, HLD, and diabetes. He presented to the ED with progressive dyspnea and fatigue. He is on LAMA/LABA for his COPD, and he does not frequently have exacerbations. He has no increased sputum production or wheezing, but he has been feeling progressively fatigued and lethargic. H Over the past few weeks he has had more dyspnea on exertion, and now has it at rest too. It is a bit worse when he lies flat. He has had no weight gain or edema in his legs and has actually lost 10-15 pounds in the last 3 months. In the ED, he is newly requiring 3-4L NC, has decreased breath sounds on the right, and a CXR shows a large right-sided pleural effusion, as well as a large apical nodule with some spiculation, both of which are new from prior.
Key Learning Points
Causes of malignant pleural effusion
–Lung cancer is the most common in men
–Breast cancer is the most common cause in women
–Lung and breast cancer account for > 50% of all malignant pleural effusions
–Other less common causes are lymphoma, GU or GI tract cancer
–Remember to consider mesothelioma
Prognosis of MPE
–Malignant pleural effusion means the cancer is advanced and stage 4 by definition
–The average life expectancy after a diagnosis of MPE is 3-12 months, depending on the patient and the malignancy
Imaging and MPE
–Make sure to get a CT scan after drainage so no lesions are missed
–Ultrasound can be helpful to look for disruptions of the pleural line, loculated fluid, or pleural nodules
Pleural fluid analysis
–Make sure to send common labs (gram stain, culture, pH)
–Cell count is very important as most MPE are lymphocyte-predominant
–Triglycerides can be helpful as well (more on chylothorax in future episodes)
–Cytology is essential and makes the diagnosis. The sensitivity is 65 – 75 percent so repeat taps may be needed and you need to send at least 60 cc of fluid (often more)
–If you have high suspicion and no diagnosis after two taps, pleuroscopy and pleural biopsy is warranted
Management of MPE
–First you need to determine if the MPE is recurrent. This requires drainage and then monitoring
— The main options are repeat thoracenteses, pleurodesis, or indwelling pleural catheter. A combination can often be used, and shared decision making is essential to the determining the best option
–The three things to consider with recurrent malignant pleural effusion are:
Did the patient feel better after drainage?
Did the lung fully re-expand?
What is the best option for this specific patient to optimize quality of life and time outside of the hospital?
–In AMPLE, pleural cetehters and talc pleurodesis were compared, and both are reasonable options with equivalent outcomes on quality of life; although pleural catehters had fewer hospital days overall.
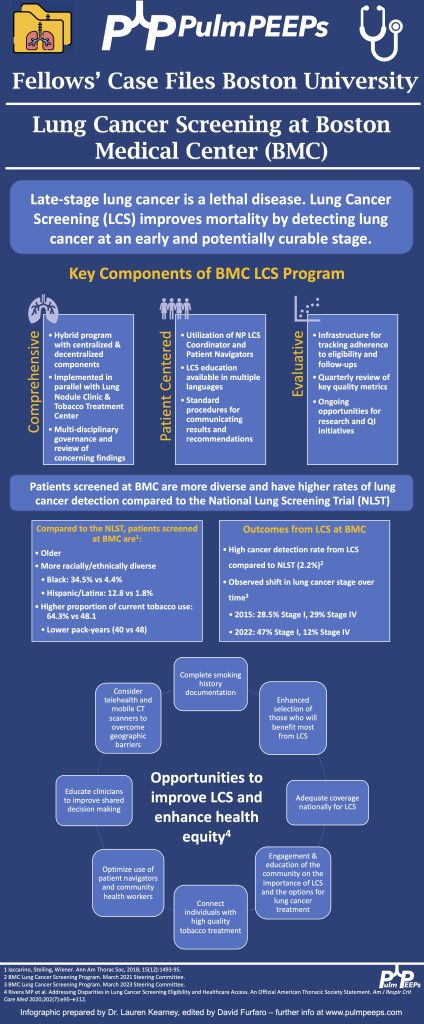
Today we’re back with another stop on our Fellows’ Case Files journey. We’re at Boston University and Boston Medical Center with an outstanding fellow, the program director, and an expert guest to dive into a new case. Tune in to hear about this fascinating case and learn some key pulmonary points along the way.
Meet Our Guests
Lauren Kearney is a research fellow at Boston University. She completed her internal medicine residency and chief residency at BU. She is pursuing a research career in health equity and community-based participatory research to improve outcomes for patients with lung cancer and other pulmonary conditions.
Chris Reardon is a Clinical Professor of Medicine at Boston University, where she is also the Fellowship Training Program Director for Pulmonary and Critical Care Medicine. She is additionally the Director of Respiratory Care Services at Pappas Rehab Hospital for Children.
Katie Steiling is an Assistant Professor of Medicine at Boston University and a Member of the Bioinformatics Graduate Program. She founded the Lung Nodule Clinic at Boston Medical Center and co-chairs the Lung Cancer Screening Steering Committee. She is dedicated to improving the equitable treatment of patients with and at risk for lung cancer.
Case Presentation
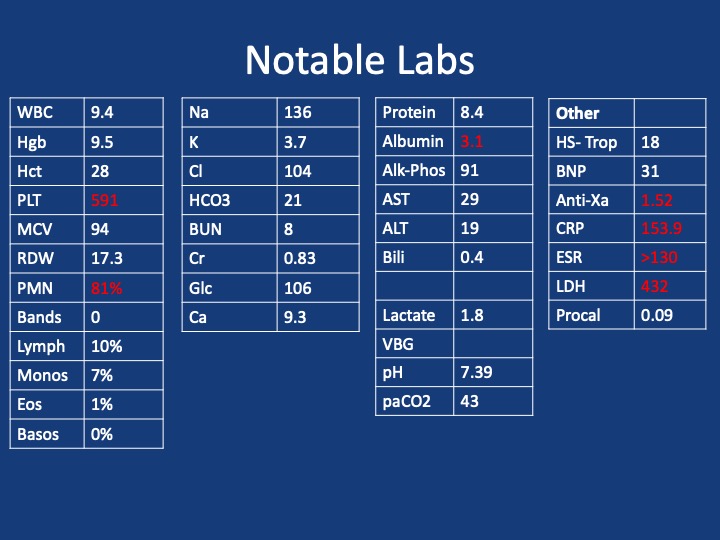
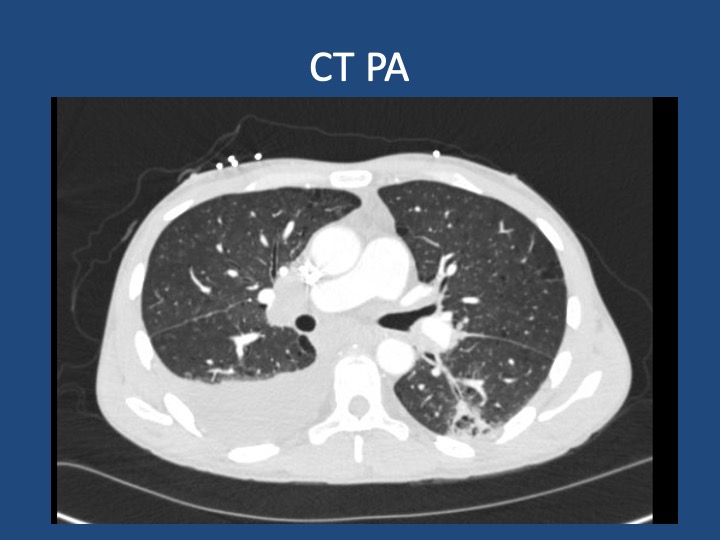
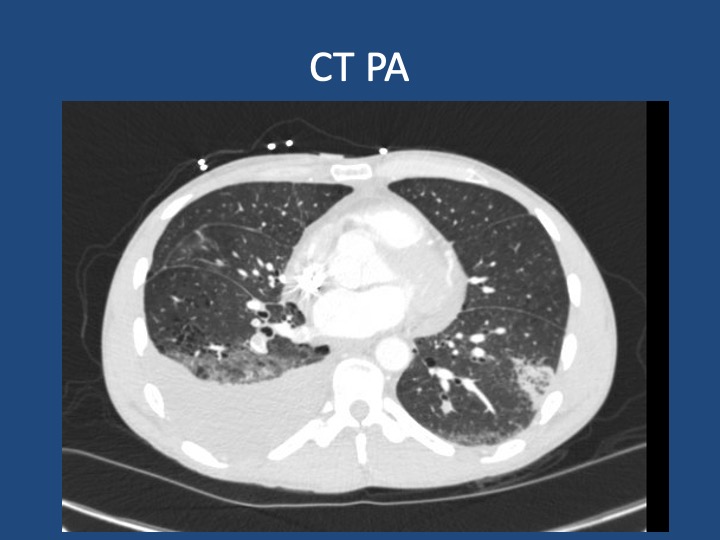
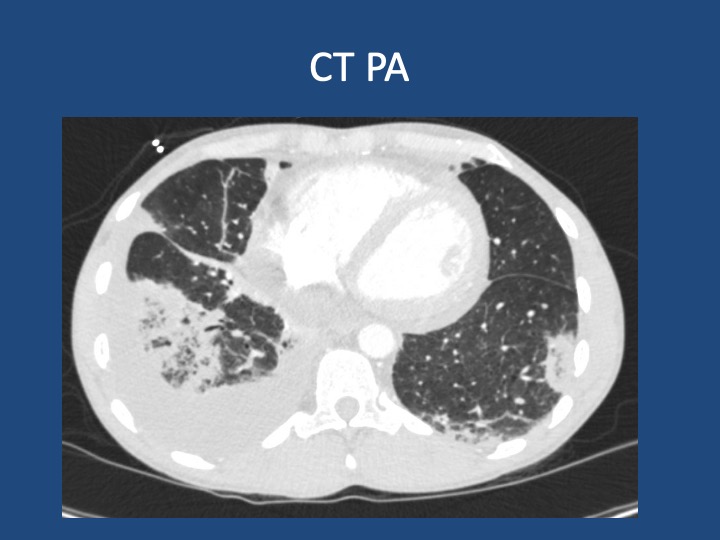
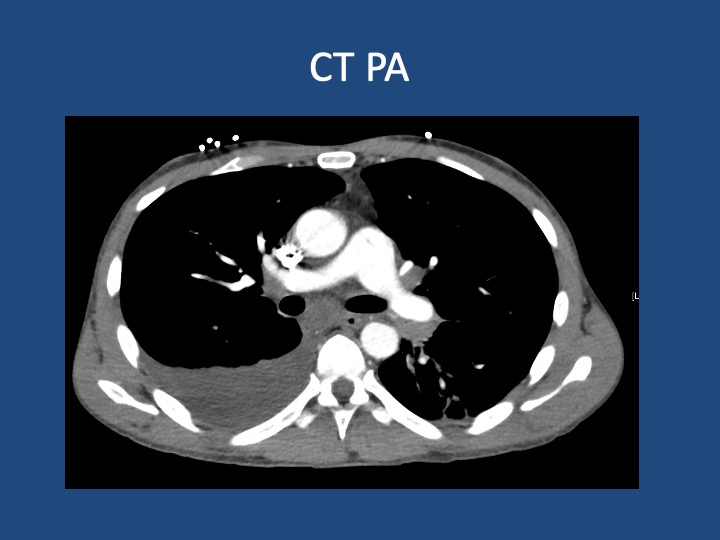
A 44-year-old man who is undomiciled and a current smoker presents with three days of intermittent, progressively worsening pleuritic chest pain with a cough productive of blood-tinged sputum. This is in the setting of 1-2 months of fatigue and anorexia, and 2 weeks of bilateral calf swelling.
Key Learning Points
Factors that may lead to initial hypercoagulability testing in first unprovoked PE: young age, thrombosis in multiple or unusual vascular beds, history of warfarin-induced skin necrosis, arterial thrombosis.
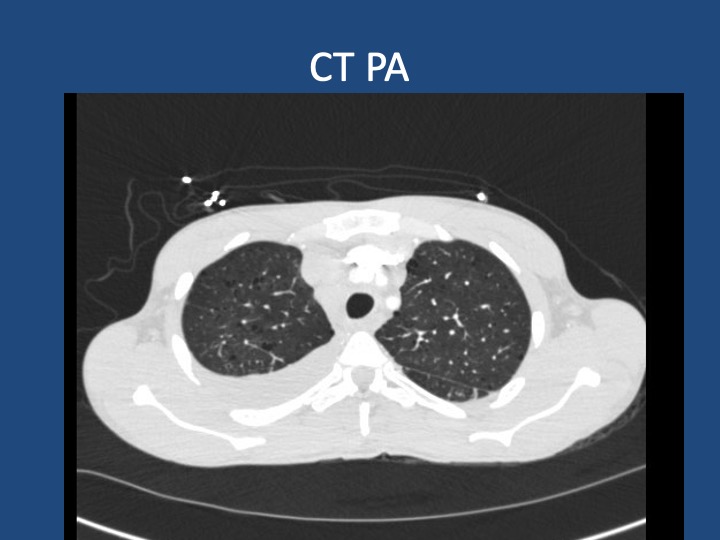
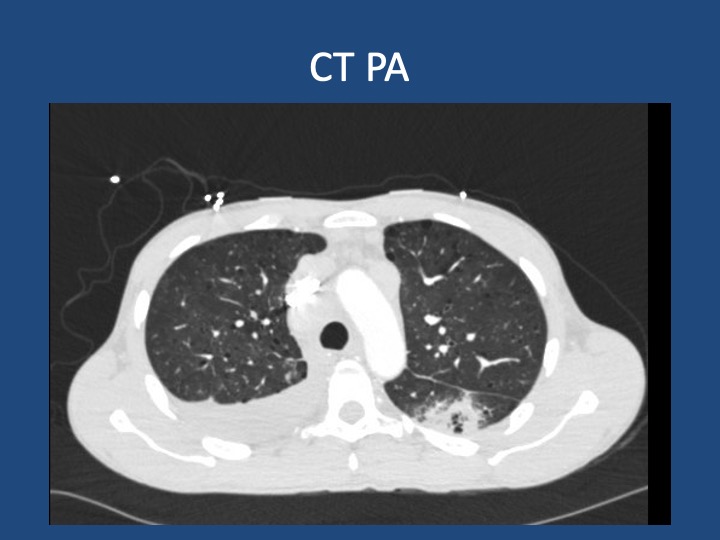
When lung cancer is suspected, identification of metastases to identify the highest radiologic stage and optimal biopsy site is essential.
Given that pleural fluid sensitivity is only ~46%, negative cytology should not assuage further malignancy work-up in a high-risk patient.
Black individuals in the US are at higher risk of developing and dying of lung cancer- the reasons for which are complex & multifactorial. Yet, gaps remain in the targeted identification of these patients, adequate lung cancer screening, and connection to diagnosis & treatment.
We are thrilled to spend time with Dr. Jessica Zitter who is an expert in critical care and palliative care medicine, author, speaker, and documentary filmmaker. We are honored to have her join the show today to discuss her work on improving end-of-life and humanistic care as well as promoting conversations about death and dying.
Meet our Guest
Dr. Jessica Zitter received her medical degree from Case Western Reserve University Medical School, and her MPH from UC Berkeley. She completed her IM residency at BWH, her pulmonary and critical care training at UCSF, and is additionally board certified in Palliative Care. She is an author of multiple essays and articles that have appeared in publications ranging from the NY Times to the Journal of the American Medical Association, has authored a book, and is a documentarian whose work is Emmy and Oscar nominated.
Dr. Zitter’s first book, Extreme Measures: Finding A Better Path to the End of Life, offers an insider’s view of intensive care in America today and its impact on how we die. Her work is featured in the Oscar and Emmy-nominated short documentary Extremis, available to view on Netflix. She has also produced and directed the award-winning, 2020 short documentary Caregiver: A Love Story. Dr. Zitter is currently working on her third film, The Chaplain of Oakland, which explores the devastating problem of racial healthcare inequities at the end of life. She has also founded the production and education non-profit, Reel Medicine Media.
Learn about the history behind the Glaucomflecken name, the inspiration for Glaucomflecken videos as well as the advocacy work they are doing. Make sure to also check out their new podcast, Knock, Knock, Hi!
Meet our Guests
Kristin Flannary completed her undergraduate work at Texas Tech University and obtained a graduate degree from Dartmouth after training in cognitive neuroscience and social psychology. She has worked as an advocate and educator for survivors of critical illness, and for the families and partners of survivors. She co-founded Glaucomflecken with Will and has received multiple awards for her work in resuscitation science, including the AHA 2022 Resuscitation Champion award.
Will Flannary completed his undergraduate at Texas Tech University, and his MD at Dartmouth. He completed his residency in ophthalmology at the University of Iowa, and currently is an Ophthalmologist at EyeHealth Northwest in Portland, Oregon. During his education and training he was diagnosed with testicular cancer, a recurrence, and then suffered a cardiac arrest, for which Kristin, quickly acted. After surviving all of this with tenacity and a strong sense of humor, he has transformed his hilarity into multiple successful comedic initiatives about medical training
We are extremely excited to be hosting this episode in collaboration with CardioNerds! We have known Amit and Dan for many years, and they have been huge supporters of Pulm PEEPs, so it is an honor to address a topic we’re all interested in together.
We are joined by experts in the field today to discuss acute, decompensated right ventricle failure in patients with Pulmonary Arterial Hypertension (PAH). This topic can be quite intimidating, so we hope this will serve as a valuable guide for anyone who encounters a patient like this in the ICU.
Meet Our Guests
Leonid “Leon” Mirson is an internal medicine resident at the Johns Hopkins Hospital Osler Medical Residency and an Associate Editor here at Pulm PEEPs. He was born in Ukraine and moved to Philadelphia in early childhood with his family. He received his undergraduate degree from the University of Pittsburgh where he studied biomedical engineering and received his medical degree from the University of Pittsburgh School of Medicine. His current interests include pulmonary and critical care medicine with a focus on pulmonary hypertension as well as medical education. He is a rising PCCM fellow at the University of Pennsylvania.
Bhavya Varma completed her medical school at the University of Pittsburgh, her internal medicine residency at Johns Hopkins, and is a rising Cardiology fellow at NYU. She is interested in medical education and has done work with CardioNerds during her residency.
Mardi Gomberg-Maitland is a Professor of Medicine at George Washington University. She serves as the Medical Director of the Pulmonary Hypertension Program at George Washington Hospital. She completed her medical degree at Albert Einstein College of Medicine, completed her residency at the Weill-Cornell Medical Center, and completed her fellowship in cardiovascular diseases at Mount Sinai Medical Center. Her research focus is on understanding the epidemiology of pulmonary hypertension and the development of novel therapeutics and biomarkers. Dr. Gomberg-Maitland is internationally known for her work, she has had extensive grant funding and has published over 150 articles, abstracts, reviews, and chapters.
Rachel Damico is a pulmonologist and an Associate Professor of Medicine at Johns Hopkins Hospital, where she is also the Associate Director of the physician-scientist training program. Dr. Damico received her medical degree and doctoral degree in Molecular and Cellular biology from the University of Pennsylvania. She completed her residency in the Osler Internal Medicine training program and continued on as a PCCM fellow at Johns Hopkins. She has quickly achieved an international reputation in the field of pulmonary vascular biology and both basic and translational research, as well as clinical excellence, in Pulmonary Arterial Hypertension.
Patient Presentation
A 21-year-old woman with a past medical history notable for congenital heart disease (primum ASD and sinus venosus with multiple surgeries) complicated by severe PAH on home oxygen, sildenafil, ambrisentan, and subcutaneous treprostinil is presenting with palpitations, chest pain, and syncope. She presented as a transfer from an outside ED where she arrived in an unknown tachyarrhythmia and had undergone DCCV due to tachycardia into the 200s and hypotension. On arrival at our hospital, she denied SOB but did endorse nausea, leg swelling, and poor medication adherence. Her initial vitals were notable for a BP of 80/50, HR 110, RR 25, and saturating 91% on 5L O2. On exam, she was uncomfortable appearing but mentating well. She had cool extremities with 1-2+ LE edema. Her JVP was 15cm H2O. She has an RV Heave and 2/6 systolic murmur. Her lungs were clear bilaterally. Her labs were notable for Cr 2.0, an anion gap metabolic acidosis (HCO3 = 11), elevated lactate (4.1), elevated troponin to 14, and a pro-BNP of ~5000. Her CBC was unremarkable. Her EKG demonstrated 2:1 atrial flutter at a rate of 130.
Key Learning Points
Diagnosing RV failure in patients with PH:
RV dysfunction and RV failure are two separate entities. RV dysfunction can be measured on echocardiography, but RV failure can be thought of as a clinical syndrome where there is evidence of RV dysfunction and elevated right sided filling pressures.
RV failure is a spectrum and can present with a range of manifestations from evidence of R sided volume overload and markers of organ dysfunction, all the way to frank cardiogenic shock. Most patients with RV failure are not in overt shock.
One of the first signs of impending shock in patients with RV failure is the development of new or worsening hypoxemia. Patients with decompensated RV failure approaching shock often do not present with symptoms classic for LV low flow state. Instead, hypoxia 2/2 VQ mismatching may be the first sign and they can be otherwise well appearing. Particularly because patients with PH tend to be younger, they can often appear compensated until they rapidly decompensate.
Causes of decompensation for patients with RV dysfunction and PH:
Iatrogenesis (inadvertent cessation of pulmonary vasodilators by providers, surgery if providers are not familiar with risks of anesthesia), non-adherence to pulmonary vasodilators (either due to affordability issues or other reasons), infections, arrhythmias (particularly atrial arrhythmias), and progression of underlying disease.
Patients with atrial arrhythmias (atrial flutter or atrial fibrillation) and pulmonary hypertension do not tolerate the loss of the atrial kick well as it contributes a significant amount to their RV filling and impacts their cardiac output. It is often difficult to determine if the atrial arrhythmia is a cause or effect of decompensated RV failure, but its presence is associated with a worse prognosis. Efforts should be made to re-establish normal sinus rhythm in patients with decompensated RV failure and atrial arrhythmias.
A patient’s home PH medications should never be stopped for any reason upon admission unless on the basis of recommendations by a pulmonary hypertension provider as this is often a cause of decompensation inpatient
Interpreting findings on echocardiogram:
Echo is a useful screening tool. When interpreting evidence of RV dysfunction, it is important to look at the global picture and not just one measurement.
RVSP, though commonly reported, may be of limited value when evaluating for decompensation. It’s a function of blood pressure, heart rate, and cardiac output. RVSP may even decline as shock worsens.
TAPSE is useful as a marker of RV dysfunction if it is reduced, but it is difficult to follow over time and only gives information about cardiac function around the annulus; it may be normal even when apical RV function is depressed. RV fractional area of change may be more useful for global RV function. It is important to pay attention to the RV size overall, the degree of TR, and the presence of effusion all of which are associated with RV dysfunction.
Tips regarding the interpretation of invasive hemodynamics:
Cardiac output by thermodilution is the standard way to calculate PVR. Despite the degree of TR that is typically present, it is thought to be a better representation of cardiac output than the estimated Fick calculation.
Our experts agree that routine monitoring of invasive hemodynamics for acute decompensated RV failure is likely not helpful and has significant risks. A good external volume exam or CVP off a central venous catheter + central venous saturation will likely be all you need to navigate a patient with shock secondary to RV failure. A right heart catheterization (should be only done under fluoroscopy for patients with large RVs) may be helpful if the etiology of shock is unclear.
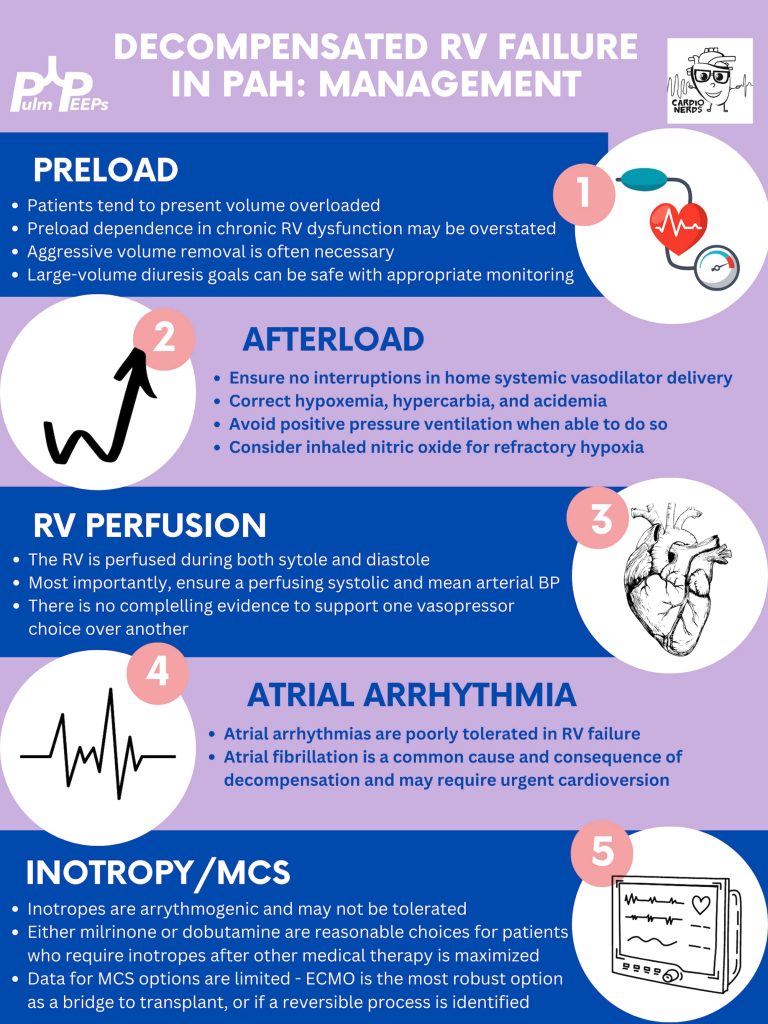
Management of decompensated RV failure in patients with pulmonary hypertension
Managing preload is of utmost importance, perhaps the most important tenant of management of decompensated RV failure. The overwhelming majority of patients with PH and decompensation are volume overloaded, it is exceptionally rare that someone would be dry. Furthermore, the myth that the RV is “preload responsive” is only true in the setting of acute RV injury (eg. RV infarction) and not so in patients with acute on chronic RV dysfunction. It is important to optimize preload in someone in decompensated RV failure and it is safe to do this more rapidly than traditionally taught. Exact goals varied between our experts, but anywhere from 2-4L net negative per day is reasonable especially if the patient is hemodynamically tolerating the fluid removal. If the patient is not responding to diuretics, hemodialysis with ultrafiltration may be necessary to optimize the patient.
Afterload is the next tenant of management. Optimizing the following parameters will reduce the patient’s pulmonary vascular resistance and reduce afterload to the right ventricle.
— Avoiding hypoxic pulmonary vasoconstriction, liberalize the patient’s O2 goal
— Avoid permissive hypercapnia and academia in this patient population
— Do not withhold a patient’s pulmonary vasodilator until discussion with the PH team. If stopped inadvertently, restart this medication immediately. For patients with malfunctioning pumps, there is a phone number on the back that you can call for rapid troubleshooting. Sildanefil can be given IV if a patient is NPO.
— Inhaled nitric oxide can improve oxygenation and reduce afterload
— Intubation and mechanical ventilation greatly increase PVR and are poorly tolerated. Exacting care must be taken to titrate PEEP and tidal volume, and avoid intubation when possible.
— Starting a new systemic pulmonary vasodilator in decompensated RV failure may be considered under close guidance from the pulmonary hypertension team
Management of atrial arrhythmias:
As above, patients with severe pulmonary hypertension do not tolerate loss of sinus rhythm well. If they are decompensated, every effort should be made to re-establish normal sinus rhythm.
Management of RV perfusion:
Unlike the LV, the RV is perfused during BOTH systole and diastole. Maintaining effective coronary perfusion to the RV is essential in RV failure. For this reason, the systemic systolic pressure (as well as the mean arterial pressure) should be kept high enough to ensure that the RV is able to perfuse. There is no great body of evidence as to which pressor works best. Norepinephrine, vasopressin, and even phenylephrine are all reasonable choices to maintain appropriate perfusing blood pressure.
Inotropy:
Patients in shock and RV failure do not always require inotropes, but if they do it’s often a sign of a grim prognosis. Either dobutamine or milrinone is reasonable, but the negative effects of these drugs (arrhythmias, tachycardia, and systemic hypotension) may limit their uses.
Mechanical circulatory support:
Limited options are available. Balloon pumps and Impella devices have limited roles except in expert centers, and ECMO remains the standard of care. ECMO (either V-V or V-A) may have utility as a bridge to recovery if a reversible cause is identified, or a bridge to transplant if the patient is on the transplant list.
Goals of care:
The prognosis of a patient admitted to the ICU with acute on chronic decompensated RV failure is guarded, with very high mortality rates even if not in shock
It is important for the patient’s longitudinal pulmonary hypertension provider to discuss the prognosis and goals of care ahead of time but this is not always possible. If they are admitted, early discussions regarding code status and prognosis are essential. It may be helpful to bring in the patient’s longitudinal pulmonary hypertension doctor into these discussions if possible.
We’re podcasting again today from #ATS2023! Yesterday, we heard all about the conference in general, with some great recaps and previews of the remaining sessions. Today, we are coming to you in collaboration with the Critical Care Assembly to preview one of the symposiums they are hosting. This session is about Cardiac Arrest: New Science and Changing Guidelines and is happening today (the day of podcast release, 5/23/23)! If you’re interested in hearing more after the episode then please plan to attend at 2:15 PM in Room 150 A-B.
For those of you who aren’t at the conference, or couldn’t make this session, we’ll talk about some of the key points and discussion topics. We will additionally be talking to the chairs of other symposiums over the next coming months so stay tuned for some more highlights from ATS 2023.
Meet Our Guest
Ari Moskowitz is an Assistant Professor of Medicine at Montefiore Medical Center / Albert Einstein College of Medicine. He is additionally the MICU Director at Montefiore Einstein and Director of Critical Care Quality Improvement. He is an NIH-funded researcher and has conducted research in cardiac arrest care, sepsis, and ARDS.
Meet our Collaborators
The American Thoracic Society Critical Care Assembly is the largest Assembly in the American Thoracic Society. Their members include a diverse group of intensivists and care providers for both adult and pediatric critically ill patients. The primary goal of the Critical Care Assembly is to “improve the care of the critically ill through education, research, and professional development.”
We are thrilled today here at Pulm PEEPs to be coming to you live from the American Thoracic Society 2023 Annual Meeting. We are joined by three fantastic speakers, and ATS leaders to discuss the highlights and events of the conference, and to share some great learning points along the way. The episode is being released immediately after recording today, Monday 5/22/23, so if you’re at the conference now make sure to listen for some extremely timely recommendations. If you’re not here in DC, we’ve highlighted some learning points that you can take away and some wisdom on how to maximize your conference experience!
We will be coming out with another episode tomorrow highlighting one of the ATS sessions, and we will continue to review symposiums from the conference throughout the year with ATS members and organizers.
Meet The Guests
Debra Boyer is a Pediatric Pulmonologist at Nationwide Children’s Hospital and has devoted much of her career to her patients and numerous trainees. Debra has been extensively involved with ATS as a prior chair of the Education Committee, and the Assembly on Pediatrics Planning Committee, and is currently on the Board of Directors and current Co-Chair of the ATS International Conference Committee.
Molly Hayes is an Assistant Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, the Director of the MICU at BIDMC, and the Director of External Education at the Carl J Shapiro Institute for Education and Research. She is also a course director for a yearly CME course on principles of critical care medicine run by BIDMC and HMS. Molly has been extensively involved with ATS as well and has served on the Education Committee, currently as a vice chair, chairs the Core Curriculum for the conference, is the chair for the Subcommittee on Education in Critical Care for the Critical Care Assembly’s Programming Committee, and has been very involved in the Section of Medical Education for the last several years.
Julianna Ferreria is an Associate Professor of Pulmonary and Critical Care Medicine at the University of Sao Paulo Medical School in Brazil, and her work focuses on mechanical ventilation. She has made a significant impact on global health initiatives and serves as the Co-Director of the MECOR program in Latin America for ATS. Julianna has also been extremely involved with ATS Critical Care Assembly Program Committee and was just awarded the Inaugural Philip Hopewell Prize for her commitment to research in low and middle-income countries.
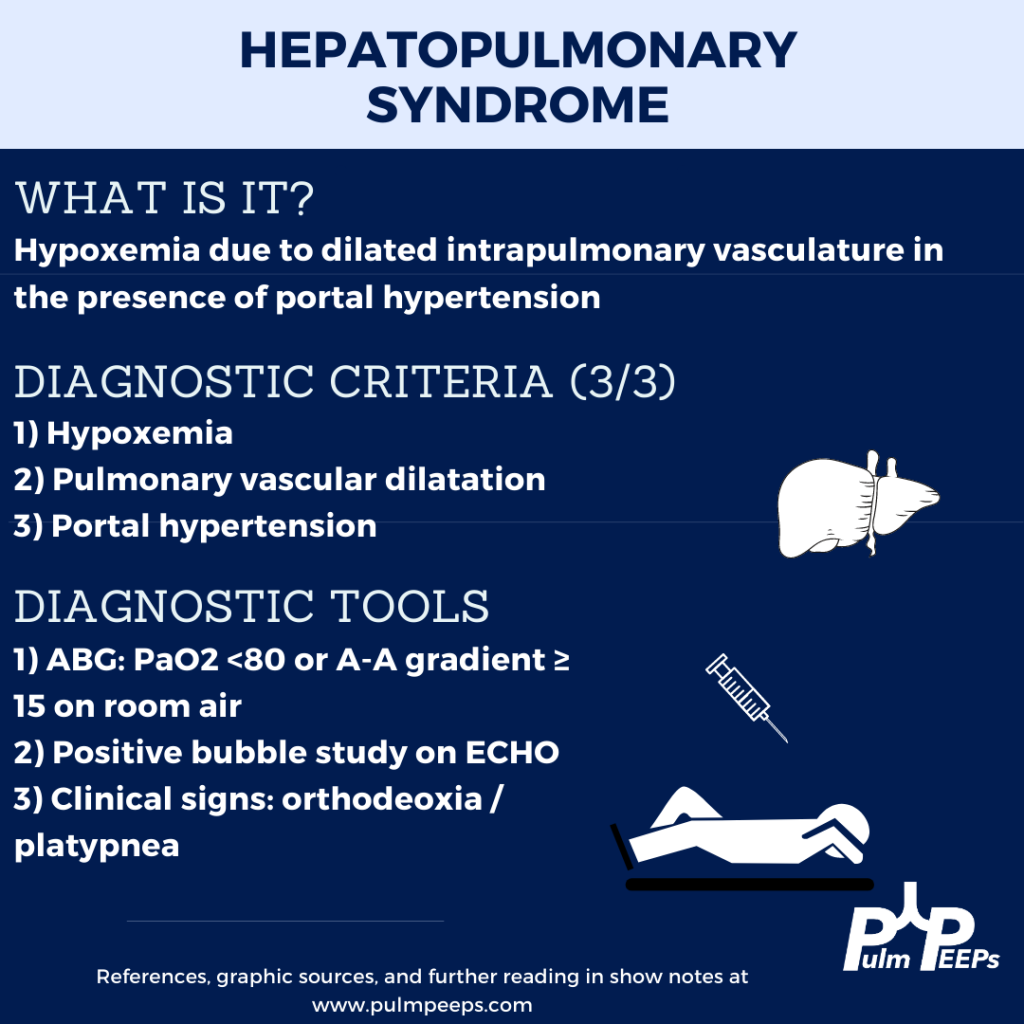
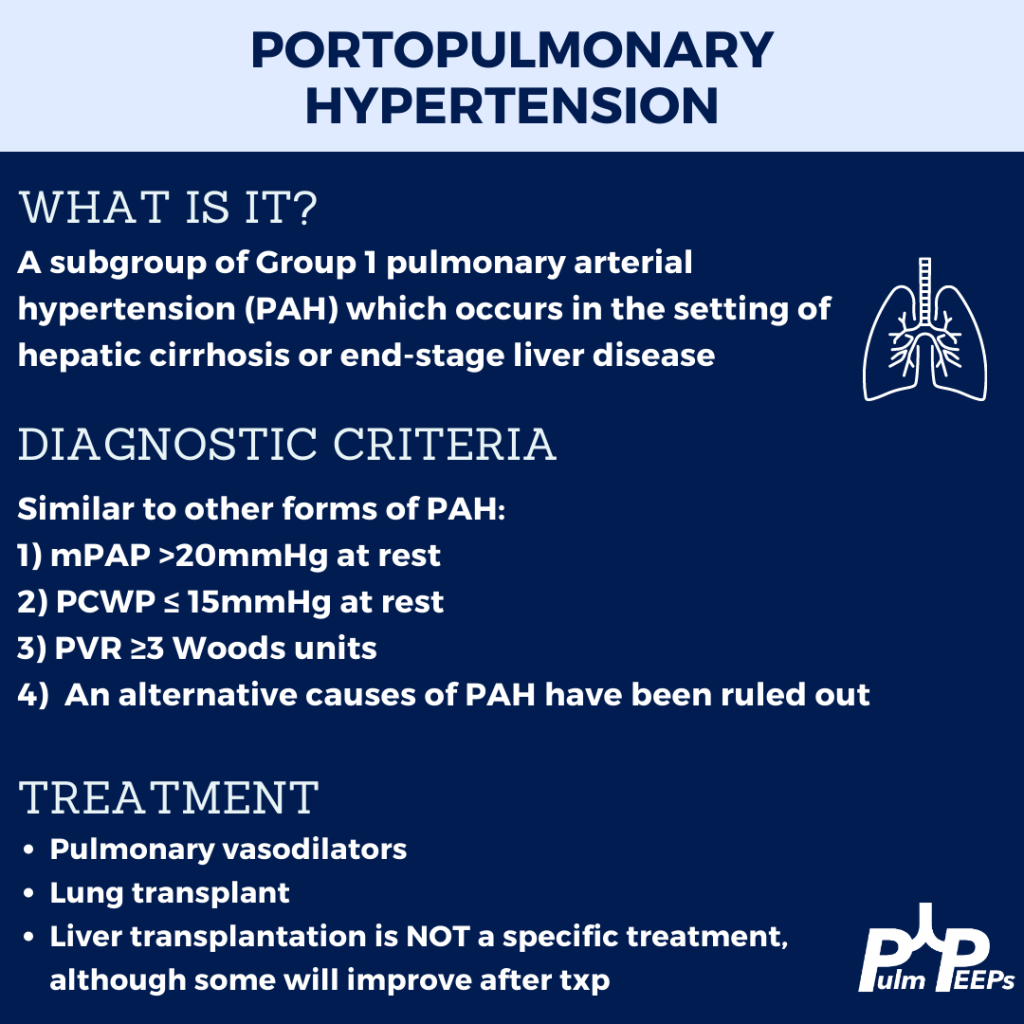
This week we are joined by one of our Associate Editors, Tess Litchman, as well as two guest experts to discuss two disease states that involve both the liver and the lung. Join us as we go through how to differentiate portopulmonary hypertension and hepatopulmonary syndrome.
Meet the Guests
Tess Litchman is a senior resident at Beth Israel Deaconess Medical Center and is one of the Associate Editors for PulmPEEPs. Tess will be continuing her training as a Pulmonary and Critical Care Medicine fellow at Brigham and Women’s Hospital next year.
Tyler Peck is an Instructor in Medicine at Beth Israel Deaconess Medical Center in the Division of Pulmonary and Critical Care Medicine. Tyler’s clinical and research interests are in pulmonary vascular disease and pulmonary hypertension.
Michael Curry is an Associate Professor of Medicine at Beth Israel Deaconess Medical Center and Section Chief of the Hepatology Department at BIDMC.
Further Readings and References
Rodríguez-Roisin R, Krowka MJ. Hepatopulmonary syndrome–a liver-induced lung vascular disorder. N Engl J Med. 2008 May 29;358(22):2378-87. doi: 10.1056/NEJMra0707185. PMID: 18509123
Krowka MJ, Fallon MB, Kawut SM, et al. International Liver Transplant Society Practice Guidelines: Diagnosis and Management of Hepatopulmonary Syndrome and Portopulmonary Hypertension. Transplantation 2016; 100:1440.
Peppas, S., Nagraj, S., Koutsias, G., Kladas, M., Archontakis-Barakakis, P., Schizas, D., Giannakoulas, G., Palaiodimos, L., & Kokkinidis, D. G. (2022). Portopulmonary Hypertension: A Review of the Current Literature. Heart, lung & circulation, 31(9), 1191–1202. https://doi.org/10.1016/j.hlc.2022.04.056