
Today’s #RadiologyRounds is a reminder that pulmonary care extends beyond the lungs! Although we’ll have a CT chest too
A 70-year-old woman with a diagnosis of seronegative RA presents with progressive dyspnea. PFTs show a moderate restrictive defect and moderately reduced DLCO. Here is the CT scan:
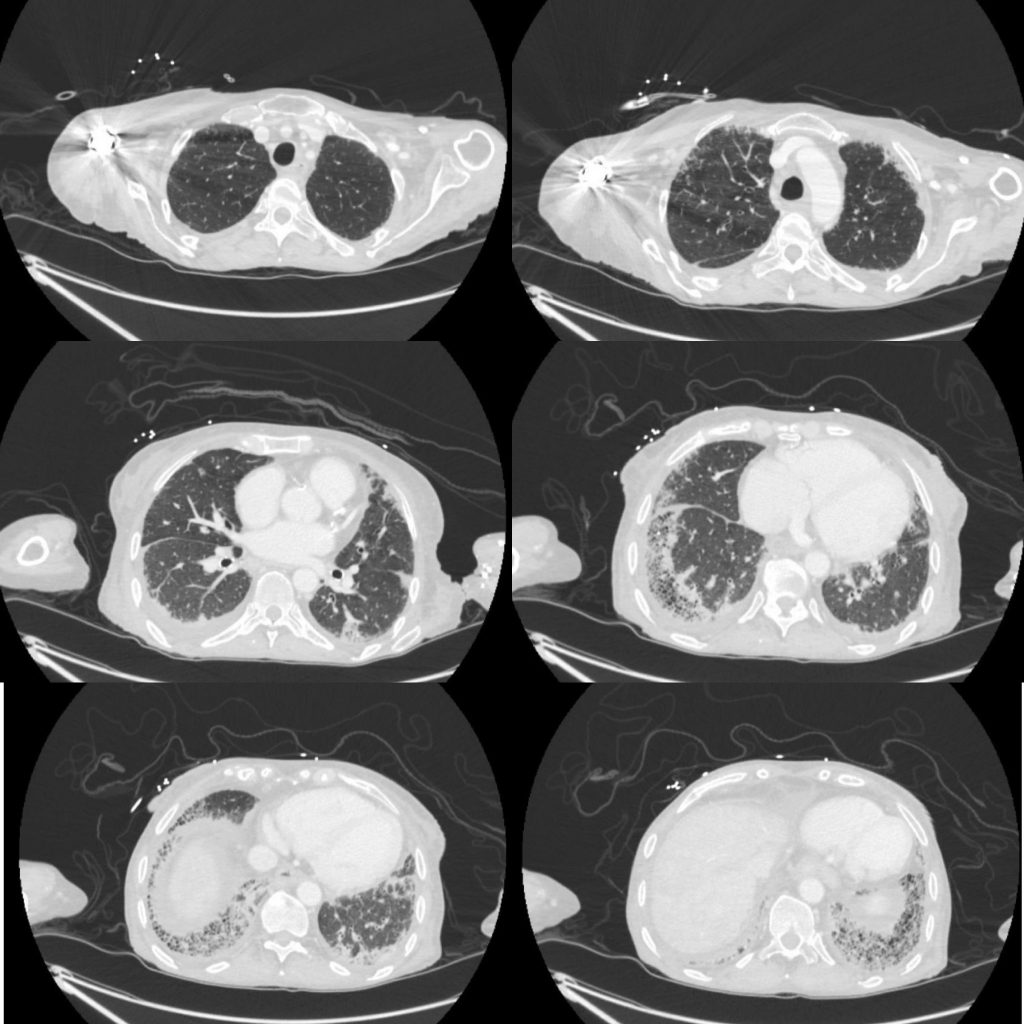
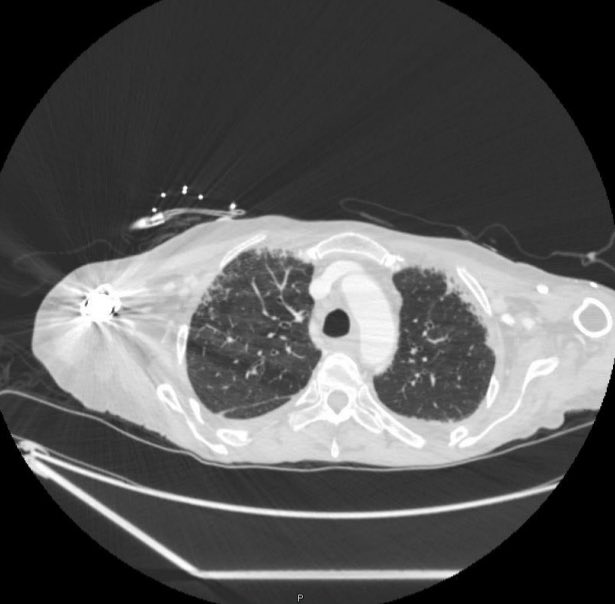
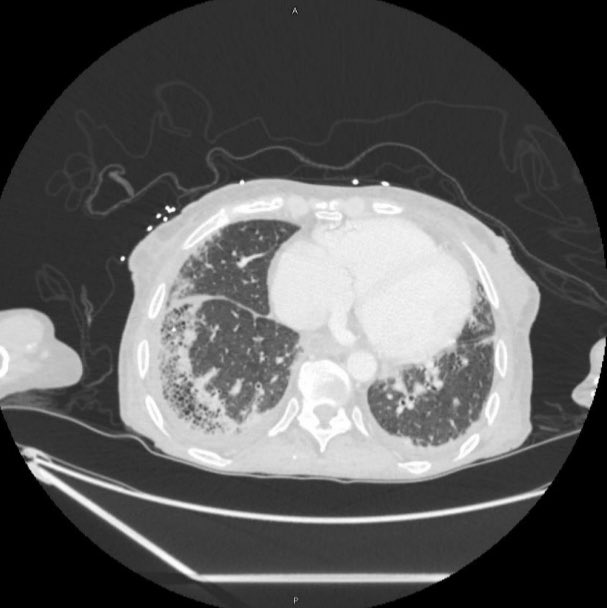
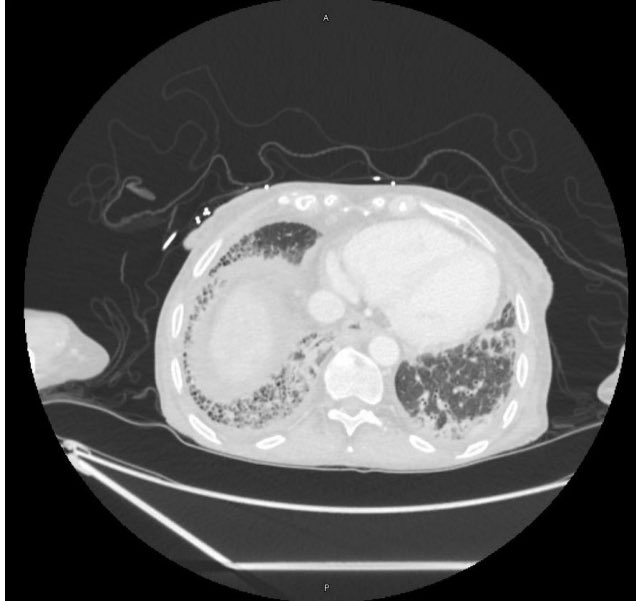
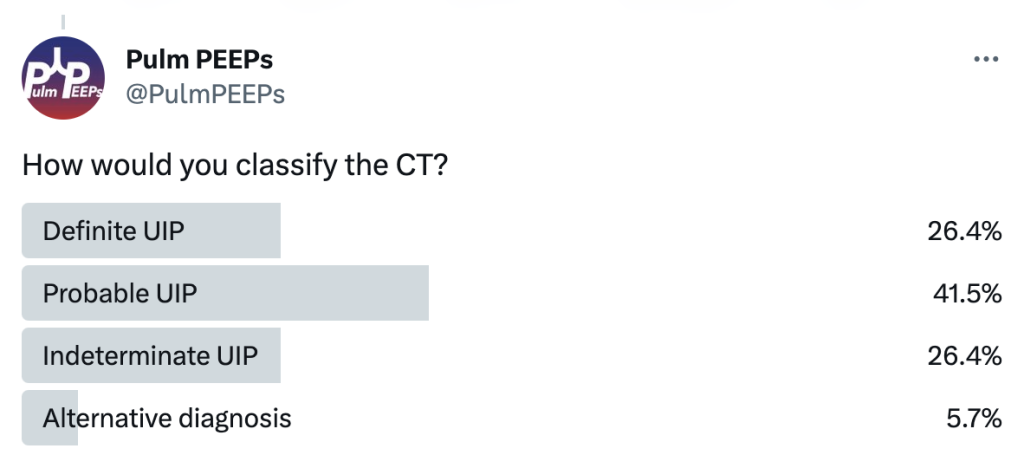
The CT was interpreted as indeterminate for UIP / fibrosing NSIP. The basilar and subpleural fibrosis and honeycombing are consistent with UIP, but with reticular nodular infiltrates and pleural effusions that are less consistent. In reviewing her history: RF, CCP, and anti-SCL70 were all negative. On hand exam, she had MCP enlargement, some PIP synovitis, and slight R hand ulnar deviation. She did not have clear telangiectasias. She had a history of GERD. She denied Raynauds. She had significant skin thickening over her legs and limited ankle mobility. X-rays were obtained:



This showed severe dystrophic calcifications and no bony erosions. This degree of extensive dystrophic calcifications is consistent with scleroderma and the patient was felt to have limited scleroderma, and possibly an overlap syndrome
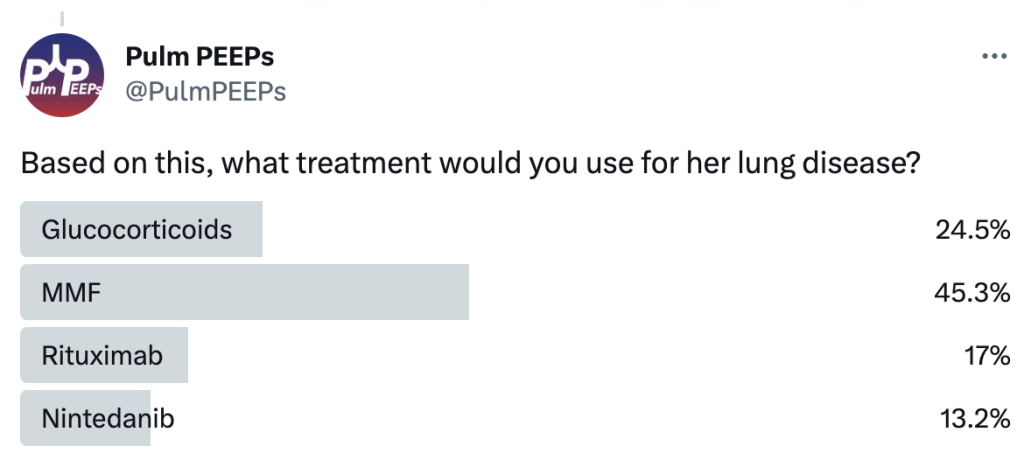
The patient was started on MMF as the initial agent based on the Scleroderma Lung Study II (SLSII): https://pubmed.ncbi.nlm.nih.gov/27469583/ Glucocorticoids were avoided given the risk of scleroderma renal crisis with steroids. An anti-fibrotic was also considered but not started as 1st line.